
Malignant melanotic nerve sheath tumours (previously known as melanotic schwannomas) are uncommon aggressive tumours commonly associated with PRKAR1A mutations and Carney complex.
On this page:
Terminology
Initially, these tumours were believed to be variants of schwannomas and were thus named melanotic schwannomas, not to be confused with conventional schwannomas that can sometimes accumulate neuromelanin 7,8.
Epidemiology
These tumours occur most often in the third through fifth decades, younger in patients with Carney complex 1,5,7,10.
Clinical presentation
Clinical presentation will depend on the location of the tumour and whether or not it has undergone malignant degeneration with metastases. As there is a predilection for spinal nerves, cord compression or focal neurology, both sensory and motor, is encountered 6. Larger peripheral lesions may merely present as palpable lumps.
Pathology
Melanotic nerve sheath tumours arise from a common precursor to both Schwann cells and melanocytes 7-9.
Over half of individuals diagnosed with these tumours have underlying Carney complex 1-3,9.
Macroscopic appearance
Malignant melanotic nerve sheath tumours appear as well-circumscribed masses of variable pigmentation ranging from grey to black, depending on the amount of melanin 3,9.
Microscopic appearance
Histologic assessment can be challenging due to heavy melanin pigmentation. The cells are variable in shape, from spindle-shaped to polygonal. They occur in two forms depending on the presence or absence of psammoma bodies, found in approximately half of cases 1-6,9:
Radiographic features
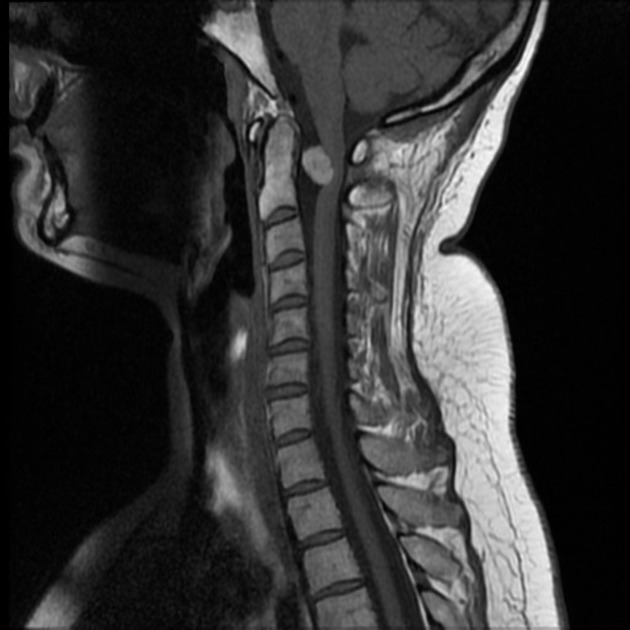
MRI
The appearances of malignant melanotic nerve sheath tumours are similar to schwannomas except that they usually have intrinsic high T1 signal and T2 signal loss due to the presence of melanin 4.
Treatment and prognosis
Although complete resection is usually curative, malignant melanotic nerve sheath tumours have a higher local recurrence rate than other schwannomas (15-35%) 3. Approximately 10% of these tumours are malignant 1,3.
Metastatic disease occurs in a significant minority and is most commonly reported in the lungs and pleura 6. Importantly, metastatic disease can be encountered even when no malignant features are identified in the primary tumour 9.
Differential diagnosis
The differential is primarily that of other neurogenic tumours and melanotic lesions including 6:
- neurofibroma
- schwannoma with haemorrhage or neuromelanin accumulation
- melanocytoma
- malignant melanoma


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}