
Marchiafava-Bignami disease (MBD) is a rare CNS disorder usually seen in the context of alcohol use and malnutrition. The condition classically involves necrosis and demyelination of the corpus callosum.
On this page:
Epidemiology
Marchiafava-Bignami disease is in most instances seen in chronic alcoholics, and as such the epidemiology reflects this demographic, with middle-aged to elderly male patients (40-60 years of age) being most commonly affected 2.
Clinical presentation
The clinical presentation of Marchiafava-Bignami disease can vary and patients often present with non-specific clinical features such as motor or cognitive disturbances, a hemispheric disconnection syndrome (apraxia, hemialexia, dementia) and/or seizures.
Pathology
The disease is attributed to a deficiency of all eight forms of the vitamin B group and results in necrosis and demyelination of the corpus callosum. Some reports present cases of extension into the hemispheric white matter, internal capsule and middle cerebellar peduncle. Although rare, Morel laminar sclerosis can also be seen 6.
Histology
Histologically, the myelin loss may be striking and may be accompanied by axonal degeneration 5.
Radiographic features
Prior to the advent of cross-sectional imaging, the diagnosis was only limited to postmortem examination and only the acute variety was diagnosed.
Marchiafava-Bignami disease typically begins in the body of the corpus callosum and later involves the genu and then splenium 2. It classically involves the central layers with relative sparing of the dorsal and ventral extremes (which may be seen as a sandwich sign on sagittal MRI).
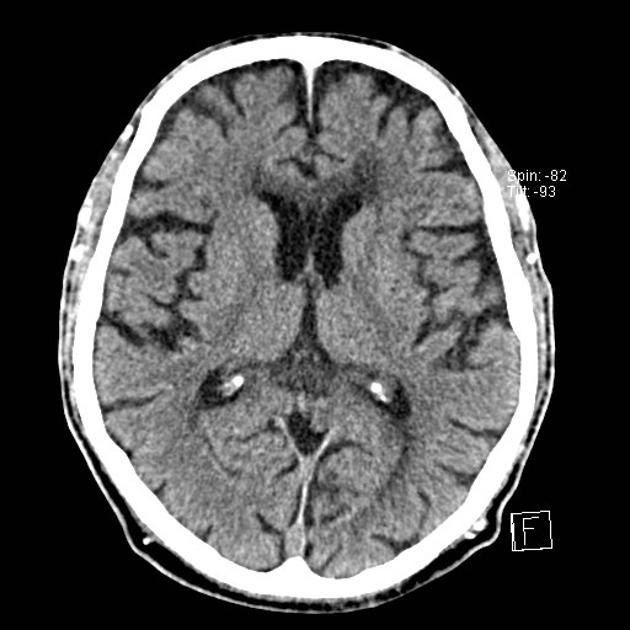
CT
may typically show hypoattenuating regions in the corpus callosum
in exceptional situations of haemorrhage, these regions may turn iso- or hyperattenuating 3
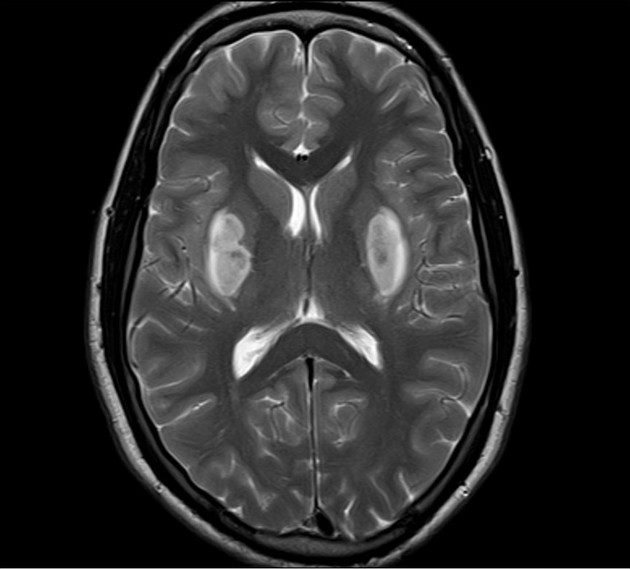
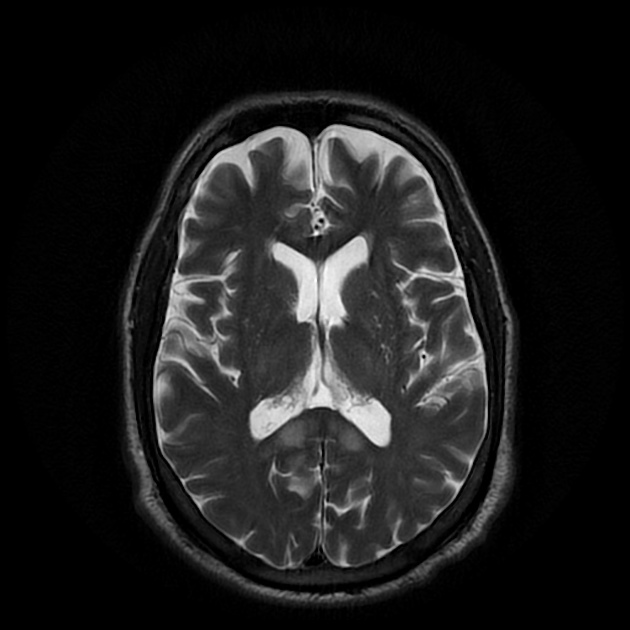
MRI
Corpus callosum may appear oedematous in the acute phase and atrophic in the chronic phase.
T1: may show hypointense foci in the corpus callosum in the acute phase
-
T2
acute phase: hyperintensities in the corpus callosum in the correct clinical setting may aid in the diagnosis
subacute phase: may show hypointense focal lesions (likely as a result of haemosiderin) 3,4
ears of the lynx sign may be seen.
MR spectroscopy: the NAA/Cr ratio may show a progressive decrease to a minimum level after the first few months followed by a partial recovery after around 11 months 3
Treatment and prognosis
Administration of vitamin B complex results in improvement in many patients, although some do not recover and may die of the disease 2.
History and etymology
The disease was originally described in Italian alcoholic patients by Italian pathologists Ettore Marchiafava (1847-1935) and Amico Bignami (1930-1994) 7,8.
Differential diagnosis
General imaging differential considerations include:
multiple sclerosis with callosal demyelination: occurs in a different clinical setting
diffuse axonal injury (DAI) to the corpus callosum: preceding trauma
callosal infarction: rare due to its rich blood supply




 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.