
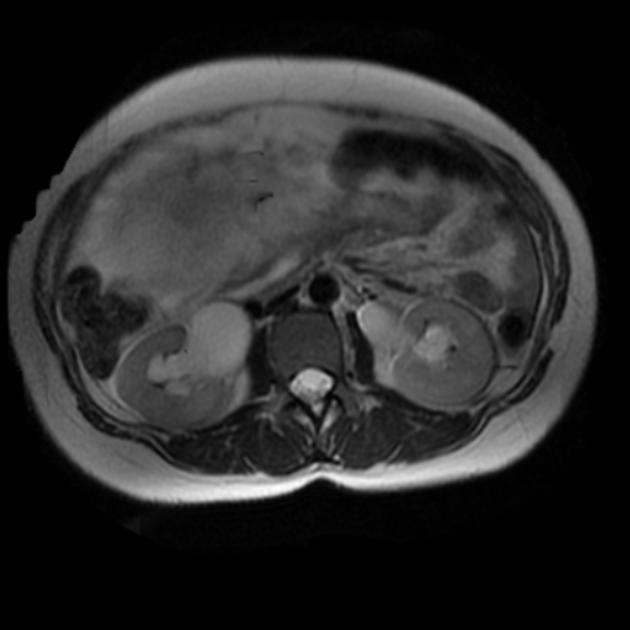
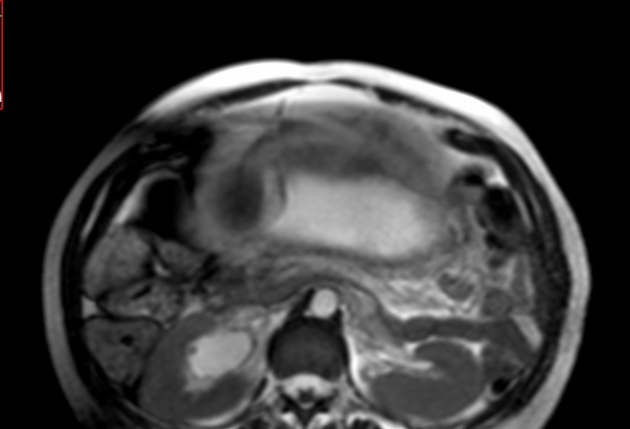
Maternal hydronephrosis in pregnancy often results as a physiological phenomenon due to the presence of the fetus.
On this page:
Epidemiology
It is estimated that up to 90% of women have some degree of asymptomatic dilatation of the renal calyces, the renal pelves and the upper two-thirds of the ureters during pregnancy 3. It is thought to be most pronounced in primigravid females.
Pathology
As the fetus grows, the dilatation usually develops during the second trimester. Mechanical compression of the ureter between the gravid uterus and iliopsoas muscle is generally thought to be the mechanism 5,6,8.
Very rarely other entities such as urinary tract calculi can complicate the picture. The prevalence of ureteric calculi in pregnancy is low and is estimated around 0.03-0.4% depending on the population.
Associations
There may be an association between gestational hydronephrosis and increased frequency of ascending urinary tract infection.
Laterality
The dilatation is often more prominent on the right side.
Radiographic features
Ultrasound
Will show renal pelvic and proximal dilatation. In order to differentiate pure physiological hydronephrosis from a worsening of an existing hydronephrosis due to an underlying pathology (e.g. urinary tract calculus), some authorities have devised charts showing the upper limit of normals allowable for gestation.
Treatment and prognosis
In most cases, it disappears within a few weeks after birth. The vast majority of asymptomatic cases are treated conservatively 1 especially since most cases of physiological calyectasis do not impair renal function. Ureteral catheters may be introduced in selected symptomatic cases. If however the kidney is obstructed with superimposed infection, prompt surgical decompression is warranted in addition to antibiotic therapy.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.