
MR enterography (MRE), also known as MRI small bowel study, is a non-invasive technique for the diagnosis of small bowel disorders.
Note: This article is intended to outline some general principles of protocol design. The specifics will vary depending on MRI hardware and software, radiologist's and referrer's preference, institutional protocols, patient factors (e.g. allergy), and time constraints.
On this page:
Indications
MR enterography, in an analogous way to CT enterography, is used to evaluate patients with inflammatory bowel disease. It demonstrates changes associated with acute inflammation during exacerbation of the disease as well as its complications such as stricture and fistula. Other indications include celiac disease, postoperative adhesions, radiation enteritis, scleroderma, small bowel malignancies, and polyposis syndromes. It is also used as alternative to small intestinal series and CT enterography.
Advantages
excellent soft tissue contrast resolution
images can be acquired in customized planes
Disadvantages
longer scanning time
more susceptible to motion and breathing artifacts
MRI incompatible implants or devices may preclude the scan
contraindicated to claustrophic patients
Technique
Patient preparation
-
light meals and clear liquids a day before the scheduled MRE
food residue may obscure lesions like polyp; hence, a low residue diet may reduce false negative findings
fasting for 4 hours prior to the study but medications with sips of water may be allowed
patient will be asked to drink a total of 1.5-2 L of fluid at regular intervals over a period of 40 or 60 minutes prior to image acquisition
-
fluids such as 1.5 L apple juice mixed with 30 mL mannitol, or 2.5% mannitol solution may be used
-
hyperosmolar fluid preparation draws fluid into the bowel and promotes bowel distension
distended bowel promotes better assessment
-
provides biphasic improved MRI soft tissue contrast:
low signal intensity on T1-weighted images
high signal intensity on T2-weighted images
-
-
instruct patient to micturate before scanning
-
empty bladder provides comfort during scanning
remember: a comfortable patient is a cooperative patient
-
-
intravenous administration of scopolamine butylbromide immediately before scanning
scopolamine reduces peristaltic movement of the intestines and mucosal folding, thus reducing artifact in the images
patient may be scanned in supine or prone position depending on institution protocol
Sequences
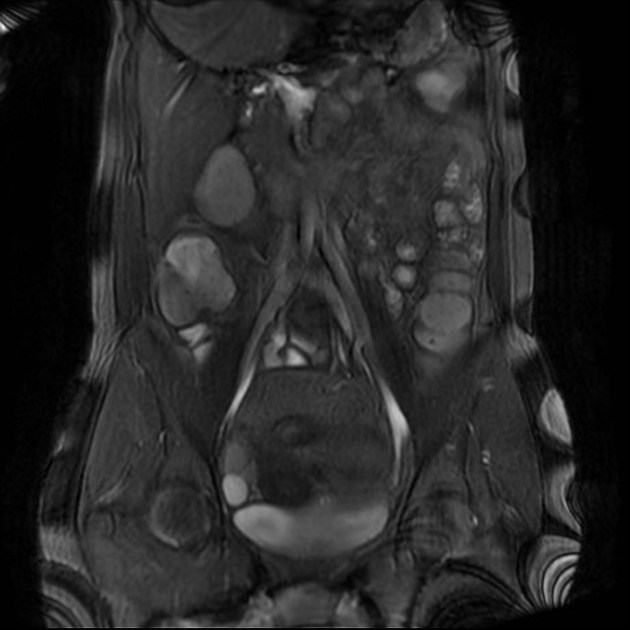
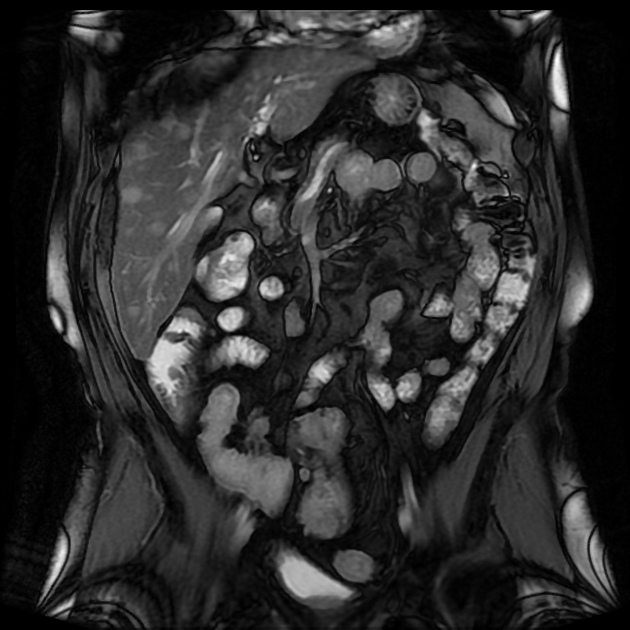
comprehensive MR examination of the small bowel usually requires axial and coronal T1 and T2 weighted images
high-resolution ultra-fast sequences such as true fast imaging with steady-state precession (true FISP)
HASTE sequence or other T2 with fat suppression
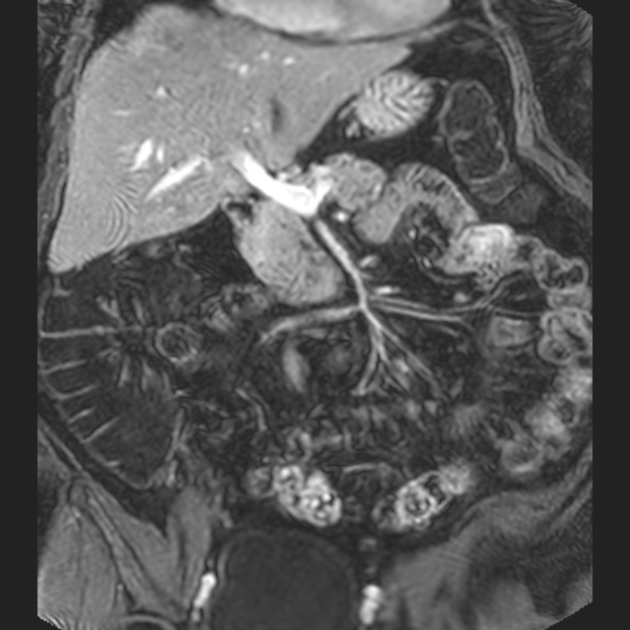
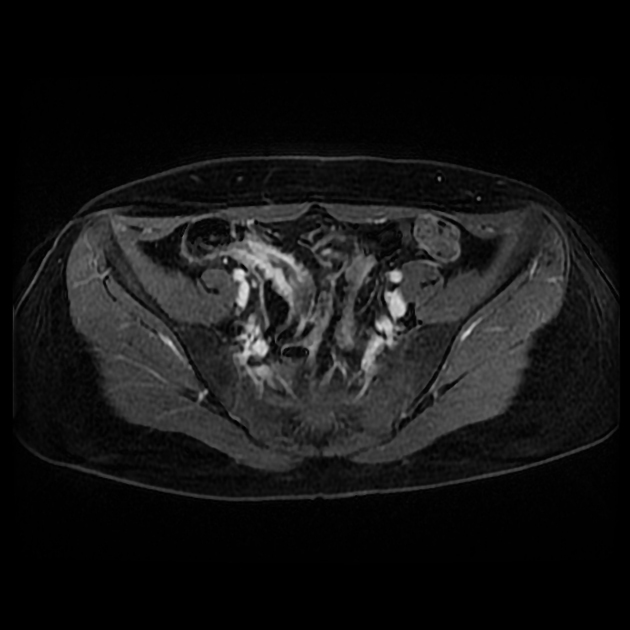
fat-suppressed three-dimensional (3D) T1-weighted breath-hold gradient-echo images of the abdomen and pelvis before and after intravenous gadolinium-based contrast material administration





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}