
Necrotising otitis externa (NOE), also known as malignant otitis externa, is a severe invasive infection of the external auditory canal (EAC) which can spread rapidly to involve the surrounding soft tissue, adjacent neck spaces and skull base.
On this page:
Pathology
Predisposing conditions for necrotising otitis externa include diabetes and immunosuppression (i.e. diabetes or patients receiving chemo- and/or radiation therapy), and is usually seen in elderly patients. Pain can be out of proportion for typical otitis externa.
Pseudomonas aeruginosa is the pathogen in 98% of cases. The route by which the infection spreads is variable. It can spread anteroinferiorly to involve the suprahyoid neck spaces (parotid space and masticator space). Alternatively, the infection can also erode the cartilaginous-bone of the external auditory canal resulting in a direct intracranial spread with resultant serious intracranial complications.
Serious complications include:
skull base osteomyelitis (some publications have used conditions as the same spectrum as necrotising otitis externa 6)
temporomandibular joint involvement
carotid artery pseudoaneurysm (secondary to carotid canal erosion by skull base osteomyelitis)
Radiographic features
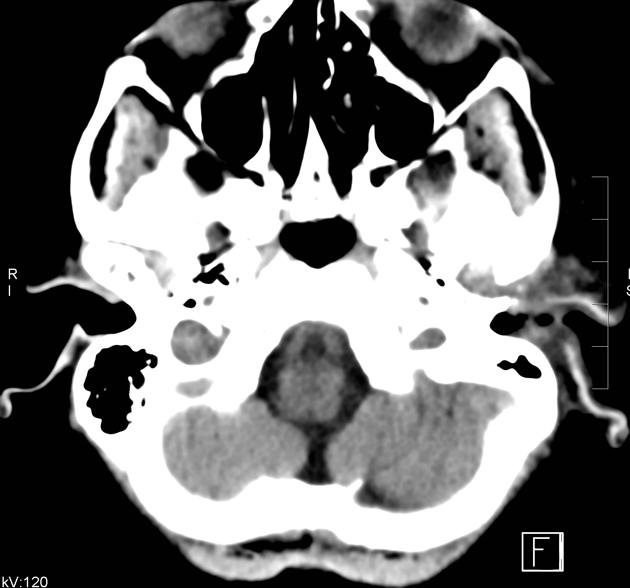
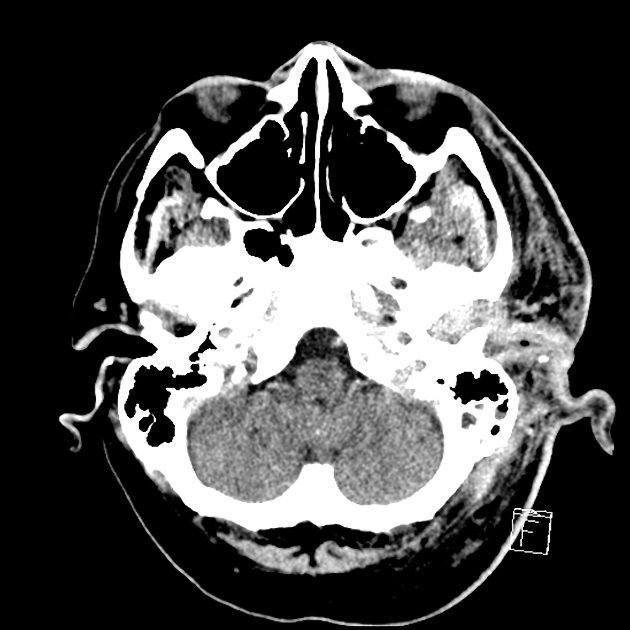
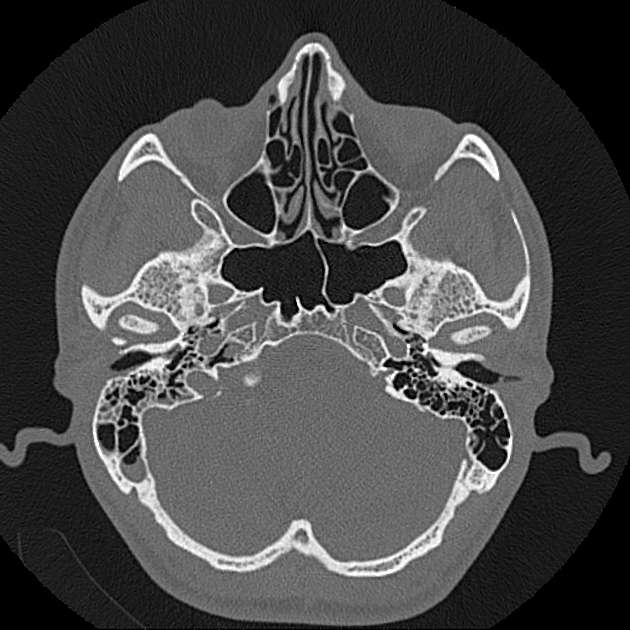
CT
On contrast-enhanced CT, there can be thickening and enhancing soft tissue and sometimes cortical bone erosion in the region of the external auditory canal with or without formation of phlegmon/abscess. In cases of abscess, cartilaginous bone ring enhancing collection with a necrotic low attenuation centre can be observed.
Necrotising otitis externa may be associated with inflammatory changes within adjacent structures such as the periauricular soft tissues, nasopharynx and parapharyngeal space. Additionally there may be opacification of the mastoid air cells and middle ear from direct extension 5.
Potential complications include skull base erosion with intracranial spread of infection.
Nuclear medicine
Technetium-99m bone scanning is sensitive to osteoblastic activity and is highly sensitive for bony infection, with uptake in the temporal bone and skull base differentiating necrotising otitis externa from typical acute otitis externa 4.
Follow up imaging using gallium-67 citrate and indium-111 labelled leucocyte scans, in addition to serum ESR levels can gauge treatment response 4.
History and etymology
The condition was first described as a disease entity by Philip E Meltzer in 1959 6 and formally clinically defined by James R Chandler in 1968 7.
Differential diagnosis
other causes of skull base osteomyelitis, e.g. mastoiditis, iatrogenic (surgery)
squamous cell carcinoma of the external auditory canal 9
erosive otitis externa: occurs in immunocompetent, exposed bone with small sequestrum 8


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.