
Osseous surgical spinal fusion refers to spinal fusion surgery with bone grafts, bone graft supplements or bone graft substitutes.
Osseous spinal fusion eventually supplies the best stability for the respective spinal segment and most types of spinal fusion surgeries are directed to establish an environment for the development of bony bridges between the diseased and unstable vertebral segments. A way to create such an environment for an osseous fusion or bony bridge to develop is the use of bone grafts and/or bone graft substitutes which are placed on the bleeding surface of vascularized freshly decorticated bone 1. The fusion process can be divided into different temporal stages in which the following processes occur 1-5:
osteogenesis: formation of new bone cells from host or graft
osteoinduction: differentiation of mesenchymal stem cells into osteoblasts and chondroblasts
osteoconduction: new bone formation, vascularization and bone graft incorporation into the host bone
The temporal stages can be classified as follows 2,5:
inflammatory phase: recruitment of inflammatory cells osteoprogenitor cells and fibroblasts
repair stage: fibrovascular stroma formation and vascularization
bone remodeling: restoration of bone strength and thickening of the cortical bone at the fusion margin
In the interim spinal stability has to be provided by other means such as spinal instrumentation hardware.
On this page:
History and etymology
Spinal fusion surgery utilizing bone grafts is the eldest form of spinal fusion surgery. Initially, spinal surgery was performed merely with autologous bone grafts used as scaffolds together with immobilization. The first posterior cervical fusions were performed in the late 19th century by Wilkins and later by Hadra 1,6. In 1927 Foerster and 1928 Juvara and Dimitriu used fibular and tibial bone grafts to treat atlantoaxial dislocation. In 1935 Kahn and Yglesias used the first iliac autograft for osseous spinal fusion 7.
Indications
Osseous surgical spinal fusion is indicated in clinical settings, where permanent stability is the main target of the surgery for a specific structure or segment.
Contraindications
Osseous surgical spinal fusion is contraindicated in situations, where permanent fixation or stabilization of a specific segment is not necessary or can be reached with motion-preserving procedures at a similar or reduced risk.
Procedure
Spinal fusion surgery with bone graft usually involves the following procedural steps:
decortication of the spinal segment to be fused
placement of bone graft against or between the decorticated bone
Options for bone grafting material include the following 1-4:
autologous bone graft (gold standard, e.g. iliac crest, ribs, local bone source)
bone marrow aspirates (osteoprogenitor and haematoprogenitor cells)
allogeneic bone graft (donor bone, cadaver bone)
demineralized bone matrices (consisting of collagenous and non-collagenous protein scaffolds and supplemented growth factors)
bone graft substitutes (e.g. ceramics, PEEK)
In addition, there are various bone graft supplements including bone morphometric protein, growth factors, mesenchymal stem cells, synthetic peptides and gene therapy 2,3.
Complications
Complications of spinal fusion with bone grafts include complications of spinal surgery and the following 1-3:
-
autologous bone graft donor site complications
infection
seroma or hematoma formation
donor site fracture
neurovascular injury
disease transmission in allogeneic bone grafts
Radiographic features
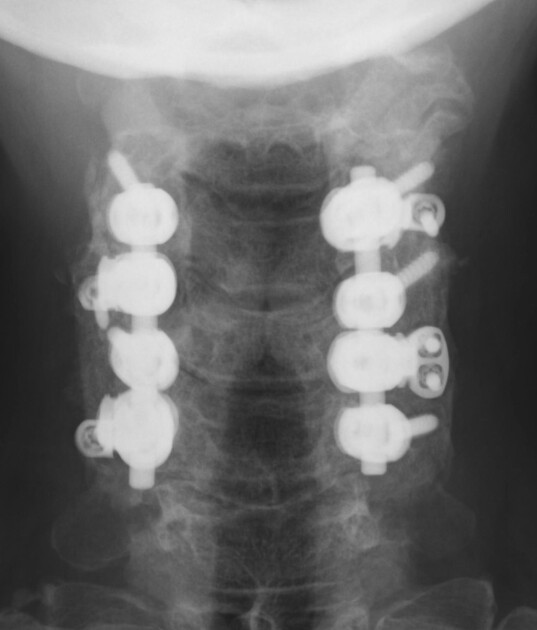
Plain radiograph
Plain radiographs are the main imaging modalities in the follow-up of spinal fusion procedures including the assessment of bony fusion and additional spinal instrumentation hardware.
Radiographic criteria of osseous spinal fusion should typically occur 6-9 months after surgery and have been defined as follows 8,9:
intersegmental position change on lateral flexion and extension views <3°
no radiolucencies around the implant
minimal loss of disk height
no fractures of the bone graft, substitute or vertebrae
no sclerotic of bone graft or vertebrae
visible bone formation in and around the implanted bone graft
CT
CT can detect and characterize osseous fusion as well as complications of spinal surgery.
MRI
MRI can be used to evaluate bony fusion and can nicely visualize and depict cancellous bone. In addition, it shows bone marrow edema and stress reactions. Depending on the additionally implanted hardware, the evaluation might be impaired by artifacts.
Radiology report
The postoperative radiological report should include a description of the following:
type of spinal fusion surgery
bone graft evaluation including bony fusion
additional implanted hardware
complications
Outcomes
Bone grafting itself as a standalone procedure lacks immediate postoperative stability and leads to an unacceptably high frequency of nonunion and pseudarthrosis of up to 40% requiring additional means of interim stabilization 1,3. Even with the use of instrumentation nonunions still occur in 10-15% of cases 3.
Autologous bone grafts have osteogenic, osteoinductive and osteoconductive properties and are characterized by slightly better fusion rates than allogeneic bone grafts.
Allografts are osteoconductive, but they lack osteogenic and have less osteoinductive properties due to the required sterilization process. However, they also require less surgical time and do not involve any donor site complications with less morbidity and faster recovery 1,2.
Bone marrow aspirates are osteogenic and osteoinductive but lack osteoconductive properties.
Demineralized bone matrices have osteoconductive properties from collagenous and non-collagenous proteins. They can be supplemented with growth factors and thus osteoinductive properties. However, they are believed to be inferior in structural composition and carry the risk of contamination during the production process 2.
Bone graft substitutes
Ceramics are cheap have long durability and can be supplemented with osteogenic cells. They lack osteogenic properties and cortical stability of autologous bone grafts 2.
Polyether-ether-ketone (PEEK) cages are characterized by better clinical and radiologic outcomes in the cervical spine and can be combined with ceramics for osteoinductive properties 2.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.