
Parotid lipomas are rare benign non-epithelial salivary gland neoplasms. They show the characteristic imaging features of fat-containing lesions and resemble lipomas that can occur elsewhere in the body.
On this page:
Epidemiology
Parotid lipomas account for 0.6-4.4% of documented benign parotid tumours 1. Mean age at manifestation of lipoma is more than 50 years and they demonstrate a predisposition for male gender 4.
Risk factors
Parotid lipomas may be related to 5:
chronic alcohol use
malnutrition with hormonal/metabolic irregularities
medication
Clinical presentation
Facial swelling, facial outline deformity and sometimes facial nerve palsy 1,4.
Pathology
Parotid lipomas are well-defined soft tissue lesions, usually encapsulated, and comprised primarily of fat. Any non-adipose segments must be carefully evaluated to eliminate a more aggressive element.
Histology
Indicates mature adipocytes with no cellular atypia or isomorphism. A thin fibrous capsule encircling a tumour of mature similarly sized adipocytes. Tumour capsule detection may benefit in differentiating such a neoplasm from lobular lipomatous atrophy and pseudolipoma all of which are non encapsulated 4.
Radiographic features
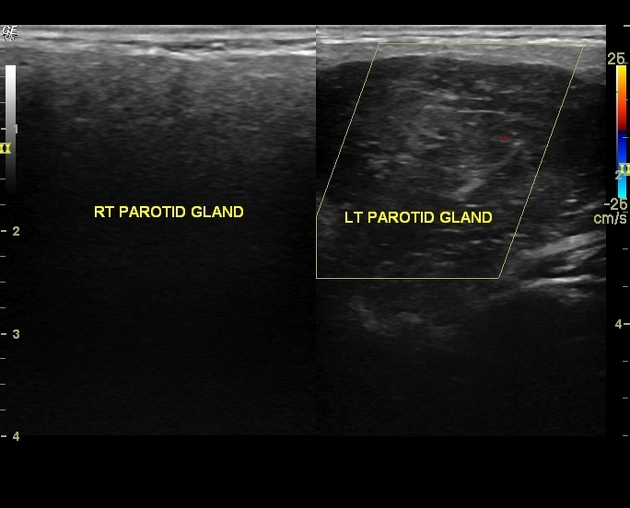
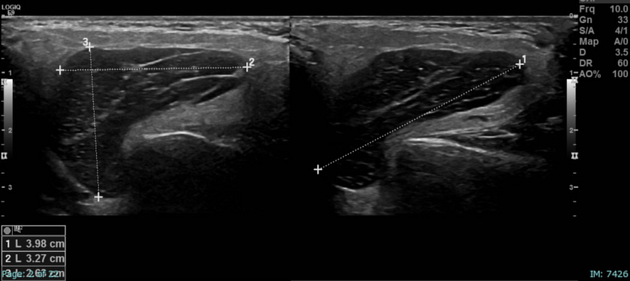
US
parotid lipomas are commonly well-circumscribed with parallel linear echogenic lines
variable appearance, hyperechoic to adjacent muscle and sometimes isoechoic or hypoechoic
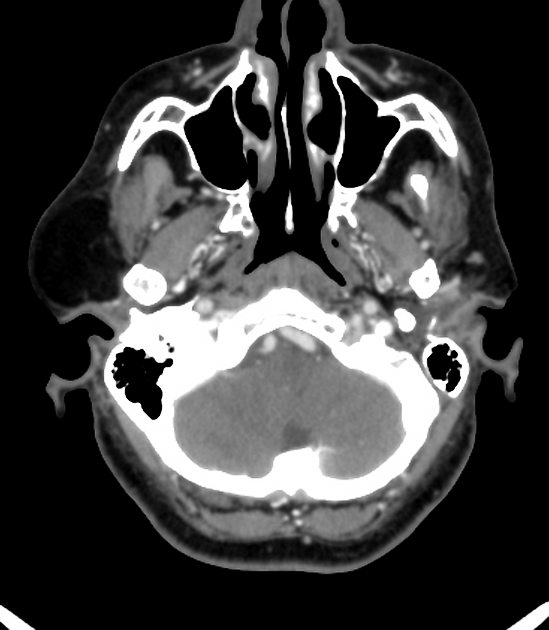
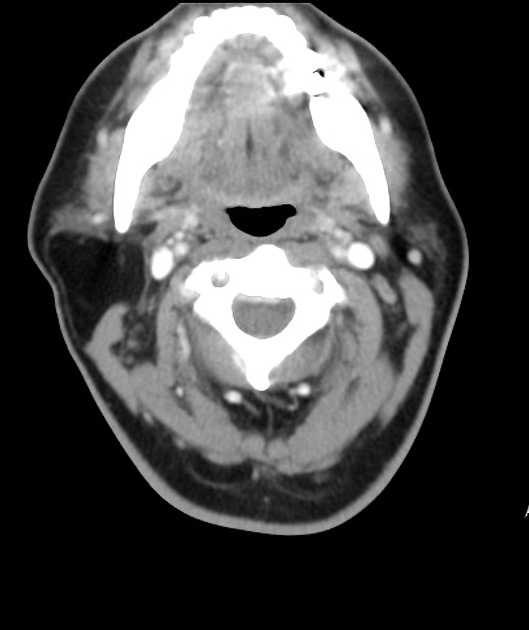
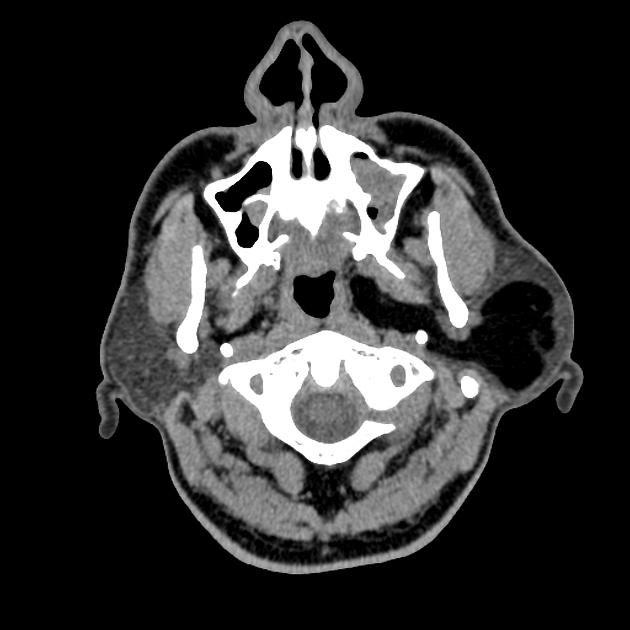
CT
lipomas retain the conventional features of homogeneous lesions with occasional septations
density of -50 to -150 HU
no post-contrast enhancement 6
MRI
MRI is the modality of choice to visualise parotid neoplasms, giving the adequate soft tissue description and repeatedly enabling visualisation of the tumour capsule from adipose tissue 3. Parotid lipomas demonstrate:
T1: high signal
T2: high signal
fat-suppressed T1: complete suppression of signal as tumours of adipocytic lineage
Differential diagnosis
lobular lipomatous atrophy
oncocytic lipoadenomas
primary or metastatic parotid masses 1






 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.