
Primary cardiac tumors are uncommon and comprise only a small minority of all tumors that involve the heart: most are mediastinal or lung tumors that extend through the pericardium and into the heart, or metastases 1.
On this page:
Epidemiology
Primary cardiac tumors have an estimated autopsy prevalence of 0.001-0.03% 2.
Clinical Presentation
The most common presenting symptoms include shortness and breath and chest discomfort, however many cases are discovered incidentally. On physical exam a characteristic auscultatory "plop" in late diastole is classically associated with left atrial myxomas of the polypoid variety 11. Other reported symptoms may include:
-
constitutional symptoms
anorexia, fatigue, fever
typically associated with myxomas
-
focal neurologic deficits
secondary to cardioembolic stroke/TIA 12
-
arrhythmogenic syncope, obstructive shock
rhabdomyomas and fibromas are associated with a predilection for malignant dysrhythmias
the former may cause a structural inflow or outflow obstruction, potentially a substrate for obstructive shock 10
Pathology
Primary cardiac tumors can then be divided into:
-
benign cardiac tumors: 60-75% 1,4
-
most common in adults, accounting for over half of benign primary cardiac tumors
-
incidence ≈10% 4, second most common in adults 6
cardiac rhabdomyoma: most common in children
cardiac paraganglioma
-
pericardial teratoma (can rapidly grow despite being benign) 7,8
-
-
-
sarcomas account for 25% of all cardiac tumors 2,6
-
most common malignant primary cardiac tumor 3,9
primary cardiac osteosarcoma: 3-9% of primary cardiac malignant tumors 9
-
primary cardiac lymphoma
-
Radiographic features
Ultrasound
Echocardiography
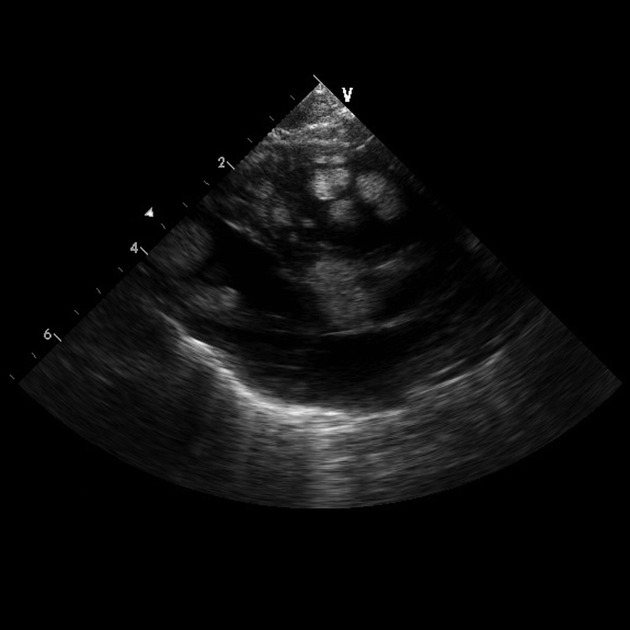
Intracardiac masses are often discovered and initially evaluated with transthoracic echocardiography (TTE) which allows delineation of the anatomic location, degree of mobility, dimensions, and any associated perturbation of cardiac structure (e.g. disruption of valvular integrity leading to regurgitation, or occlusion of the valvular orifice leading to stenosis) and function. Pericardial extension can also be delineated. Transthoracic evaluation is limited both by inherent anatomic barriers to visualization of several pertinent structures such as the great vessels, and may be further limited by patient specific factors, such as prior surgeries or dressings, chest wall abnormalities, body habitus, and hyperinflated lungs.
Transesophageal echocardiography (TEE) is particularly utile for evaluation of masses which may be related to a valvular apparatus and is superior for imaging structures within the atria. It is particularly useful for delineating the origin/attachment site of masses (commonly difficult with a transthoracic approach).
3-dimensional echocardiography (3DE) is often sought for its ability to detail the anatomical relationships of masses, provide better definition of mass shape and dimensions, and additional details subtle structural elements within the mass which would not otherwise be apparent e.g. subtle internal trabeculation.
Sonographic contrast agents may also provide additional diagnostic yield, allowing one to assess the presence of vascularity within a mass, and the relative abundance or dearth of perfusion. Typical features associated with benign tumors include qualitatively small amounts of microbubbles circulating throughout the mass (i.e. lacking the hypervascularity associated with malignancy), appearing to have a lesser degree of enhancement to the adjacent myocardium. Identification of intra-cavitary masses may also be enhanced with their presence indicated by a filling defect within the relevant cardiac chamber 14.
MRI
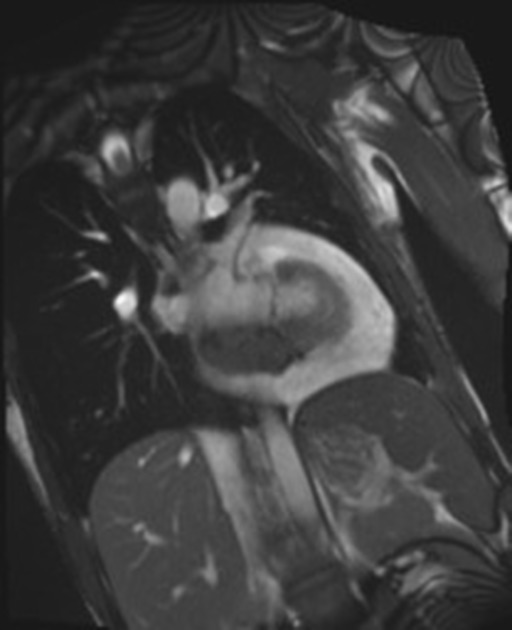
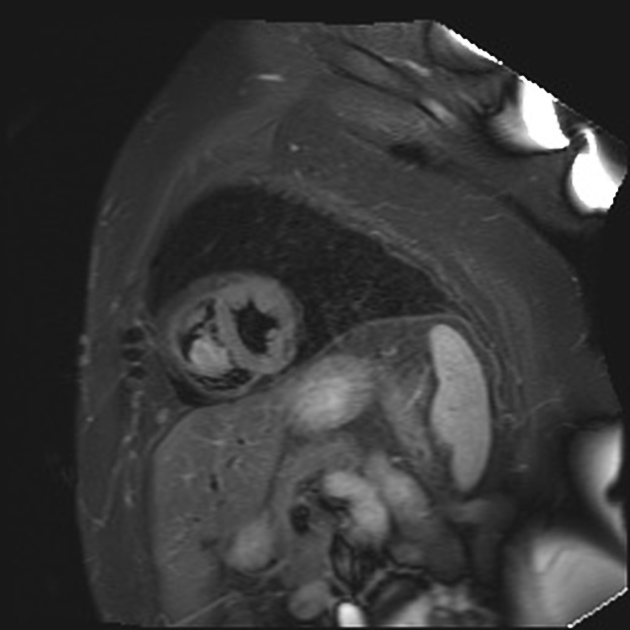
While of limited utility in structures subject to a high degree of motion (such as masses associated with a valve) cardiac magnetic resonance imaging (CMR) allows both qualitative and quantitative evaluation of the mass in question as well as cardiac structure, function, and adjacent structures 15. Features salient to assess on CMR include:
location, shape/size, involvement of adjacent anatomical structures 14
absence or presence (and degree/pattern of) late gadolinium enhancement
CT
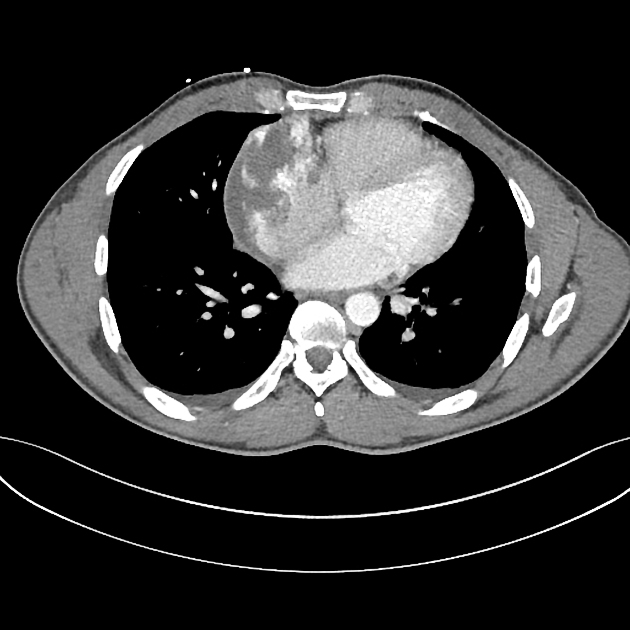
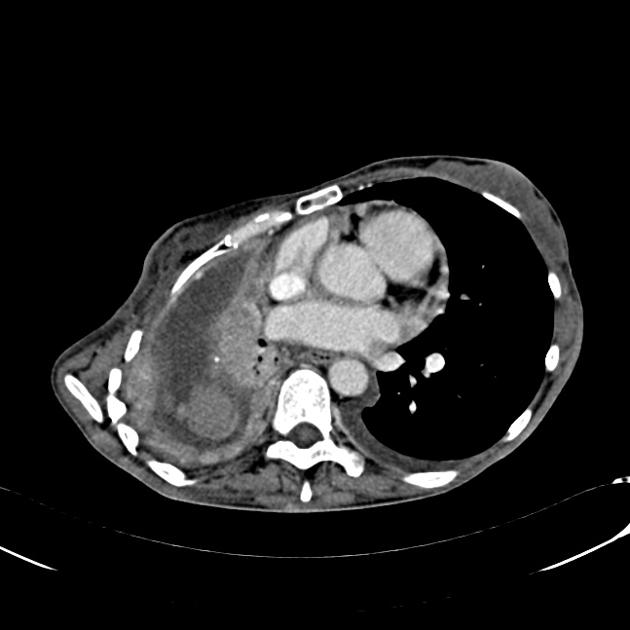
As metastases are far more common than primary tumors, computed tomography (CT) of the chest, abdomen, and pelvis may be considered to identify a primary source of malignancy, with common culprits including:
-
hematologic malignancy
lymphoma, leukemia
hematogenous seeding from melanoma may also occur
breast cancer
lung cancer
esophageal cancer
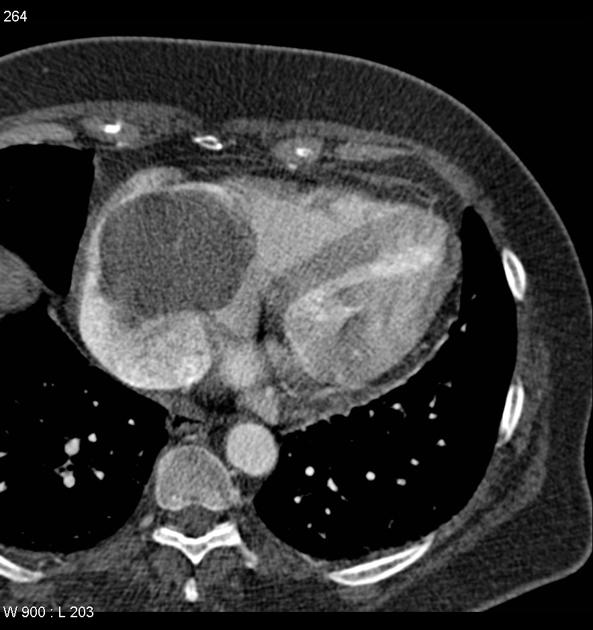
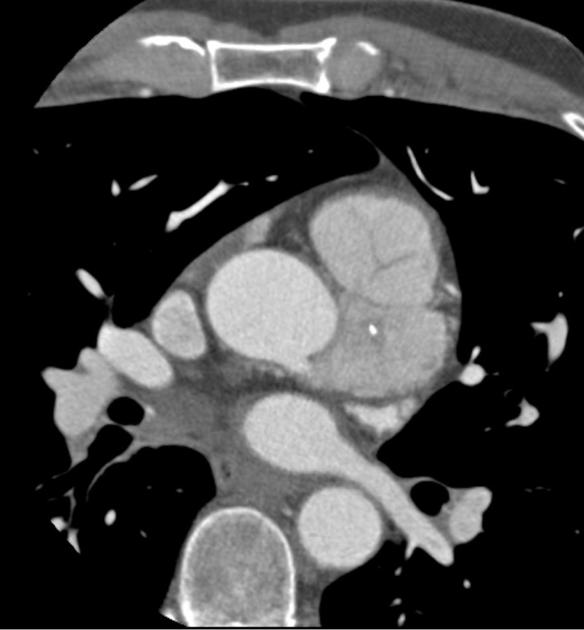
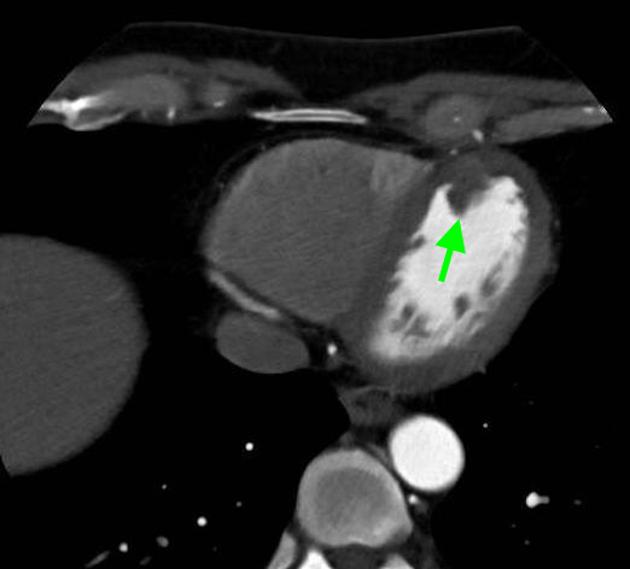
CTCA may also be implemented to evaluate masses though to involve coronary vessels and allows identification of extra-cardiac extension of a tumor into adjacent structures. Contrast enhancement allows insight into the vascular nature of the mass, and fat/calcifications are visualized well with CT 15.





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.