
Primary fallopian tube carcinoma is an extremely rare malignancy that arises from the fallopian tube. It accounts for ~1 (0.2-1.1)% of all gynecological malignancies (least common of all gynecological malignancies 3).
On this page:
Epidemiology
The estimated incidence is at ~3-4 per million women 3. It typically presents in post-menopausal females (peaks at 6th-7th decades).
Clinical presentation
Most patients are asymptomatic or tend to present with non-specific or insidious symptoms. The symptoms are complex, comprising of an intermittent profuse serosanguineous vaginal discharge, colicky lower abdominopelvic pain relieved by the vaginal discharge, and an adnexal mass (present in ~15%). This clinical constellation is termed the Latzko triad 13,14.
Pathology
The pattern of growth can be nodular, papillary, infiltrative, or mass-forming.
Location
Most primary fallopian tube cancers arise from the ampulla with endoluminal growth that leads to obstruction and distension of the fallopian tube (hydrosalpinx), which explains why the majority of these patients are rarely asymptomatic in contrast with those with ovarian cancer.
Bilateral involvement occurs in ~20% of cases, mainly in advanced disease 1.
Subtypes
-
papillary serous adenocarcinoma
most common histological subtype
can be histologically identical to a serous cystadenocarcinoma of the ovary
endometrioid carcinoma
transitional cell carcinoma
Markers
Serum CA-125 levels are often elevated 6,8.
Radiographic features
Advanced tumors are difficult to differentiate from ovarian tumors on imaging. The presence of a hydrosalpinx can be a useful feature.
Ultrasound
While being non-specific, it may be sonographically identified as a complex cystic mass involving the fallopian tube with papillary projections 10,11.
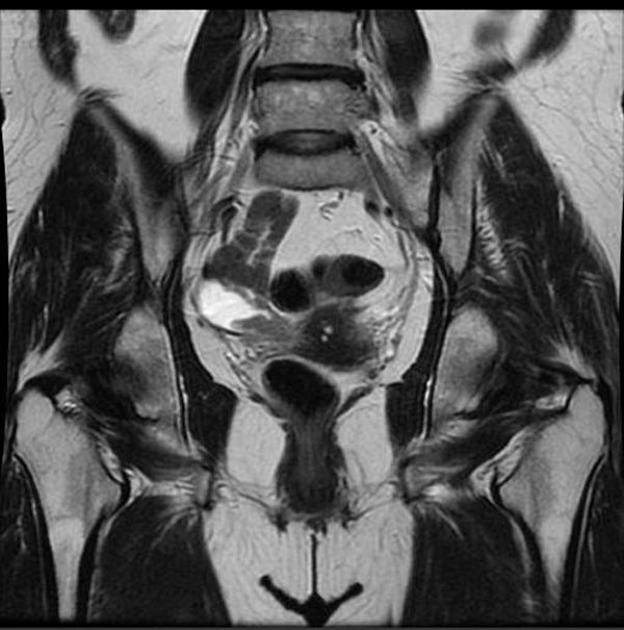
MRI
While signal characteristics are non-specific, they generally are as follows 1,3:
-
T1
solid tumor portion is usually of low signal
if there is an associated simple serous fluid containing hydrosalpinx, this may be low signal
if there is an associated simple hemorrhagic fluid containing hydrosalpinx, this may be high signal
-
T2
solid tumor component is often homogeneously or heterogeneously low or of intermediate signal
if there is an associated simple serous fluid containing hydrosalpinx, this may be of high signal
T1 C+ (Gd): solid portion often demonstrates enhancement
Staging
See staging of primary fallopian tube carcinoma
Treatment and prognosis
Compared with ovarian carcinoma, fallopian tube carcinoma tends to present at an earlier stage but has a worse prognosis, stage for stage 2. However, the better overall survival of fallopian tube carcinoma may be on the basis of an earlier stage at presentation 4. Treatment generally consists of surgical debulking followed by chemotherapy.
Differential diagnosis
For a mass involving the fallopian tube, differential considerations would be:
tubal ectopic pregnancy: women of childbearing age and elevated β-hCG
primary ovarian cancer (especially ovarian epithelial tumors) with involvement of the fallopian tubes
-
infective of inflammatory conditions


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.