
Retro-odontoid pseudotumors, also known as periodontoid pseudotumors, are non-neoplastic soft tissue masses adjacent to the odontoid process (dens) of C2, which can cause cervicomedullary compression.
On this page:
Epidemiology
The prevalence of retro-odontoid soft tissue thickening, particularly with mineralization presumed to represent calcium pyrophosphate deposition, increases significantly with age 1.
Clinical presentation
These are often asymptomatic. Acute inflammation in these masses (as in crowned dens syndrome) can manifest as neck pain or headache. As a chronic process, mass effect on the cervical spine can manifest as myelopathy including sensory and motor deficits.
Pathology
Pseudotumors can arise by various mechanisms and etiologies 2,3:
-
rheumatoid arthritis (RA): in which case it may be termed pannus
trauma
-
atlantoaxial hypermobility compensating for subaxial ankylosis
-
deposition diseases
amyloid arthropathy associated with hemodialysis
dens fracture callus
migrated disc herniation
Radiographic features
The entity is defined by soft tissue thickening at the atlantoaxial junction around the expected location of the transverse atlantic ligament, posterior to the dens.
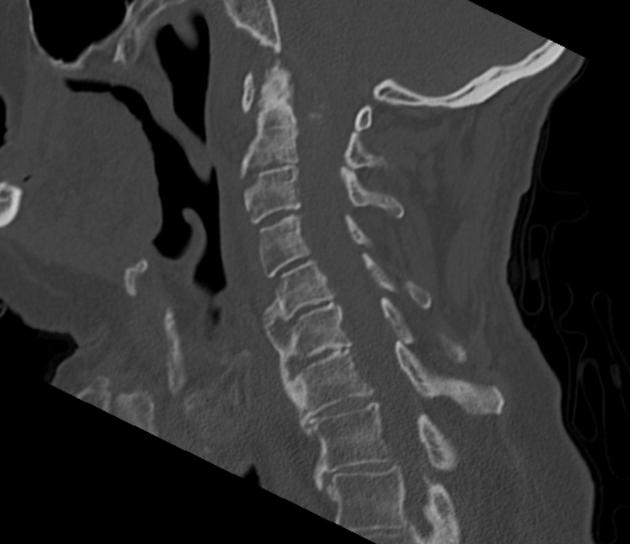
CT
Mineralization within the pseudotumor may be present in calcium pyrophosphate deposition disease (chondrocalcinosis, linear/arciform), hydroxyapatite deposition disease (cloudlike), gout (faintly), fracture callus, and ossification of posterior longitudinal ligament (by definition).
Joint or pressure erosion may be present in RA, CPPD, gout, and tenosynovial giant cell tumor.
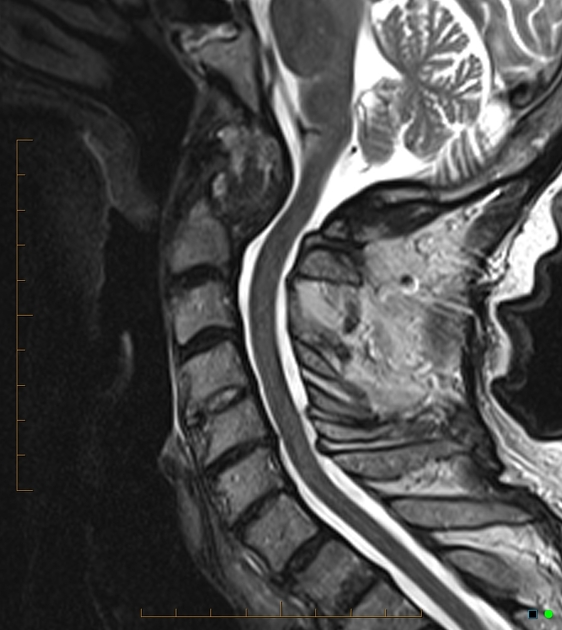
MRI
Signal characteristics vary by etiology. In general, there are no reliable imaging features that distinguish rheumatoid arthritis-related pannus from non-rheumatoid retro-odontoid pseudotumor.
T1: usually low
T2: variable, often heterogeneous
Differential diagnosis
Consider:
retro-odontoid synovial cyst





 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.