
The term trauma (plural: traumas) or traumatic injury refers to damage or harm of sudden onset caused by external factors or forces requiring medical attention.
Polytrauma or multiple trauma has been defined as a pattern of potentially life-threatening injuries involving at least two body regions.
On this page:
Epidemiology
Traumatic injuries are very common and major trauma is the leading cause of death in children and young adults 1-3 and is a major cause of deaths and disability globally with different distribution patterns beyond the age of 35 years of age 1.
Risk factors
Risk factors are diverse and include socioeconomic, occupational, political, cultural and environmental parameters 1,2.
Clinical presentation
The clinical presentation involves typical injury mechanisms as road traffic accidents, sports or work-related injuries, falls, interpersonal violence, cuts, stabs or gunshot wounds, natural disasters, burns and other injury types 1. Depending on the extent and severity of the traumatic injury patients might seek medical attention from their primary physician within the scope of a routine visit or might be found unconscious in the field and brought to the hospital by ambulance or helicopter.
Complications
There is a wide spectrum of complications resulting from traumatic injuries.
Major sequelae include 3,4:
major bleeding
trauma-induced coagulopathy
acidosis
loss of consciousness/coma
permanent disability
death
Pathology
Pathogenesis
Pathogenesis of trauma and/or traumatic injuries include:
-
physical injury
blunt injuries
thermal injury
chemical injury
electrical injury
ionising radiation injury
barotrauma
acoustic trauma
Aetiology
Causes of trauma and traumatic injuries include the following 1,2:
traffic collisions
occupational injuries
falls
recreational and/or sports-related injuries
interpersonal violence and/or assault
self-inflicted injuries
other accidents
natural disasters
Location
Traumatic injuries can occur in any conceivable location of the body.
The Abbreviated Injury Scale (AIS), which also forms a basis for the calculation of the Injury Severity Score, specifies the following locations:
head (without face)
face
neck
thorax
abdomen
spine
upper extremities
lower extremities
external injuries and other traumatic injuries
Classification
Traumatic injuries are usually classified based on their location, their extent and their severity with different classification schemes for various organs and tissues.
Based on their severity, traumatic injuries can be subdivided into the following 1:
injuries treated outside the health care system
injuries treated in primary care centres
injuries requiring emergency care
injuries requiring hospital admission
lethal injuries
In consideration of the respective tissue traumatic injuries can be subdivided into the following types:
cartilage: fissures, fractures, osteochondral injuries
muscles: contusions, tears, ruptures
tendons: tears, ruptures
ligaments: sprain, tears
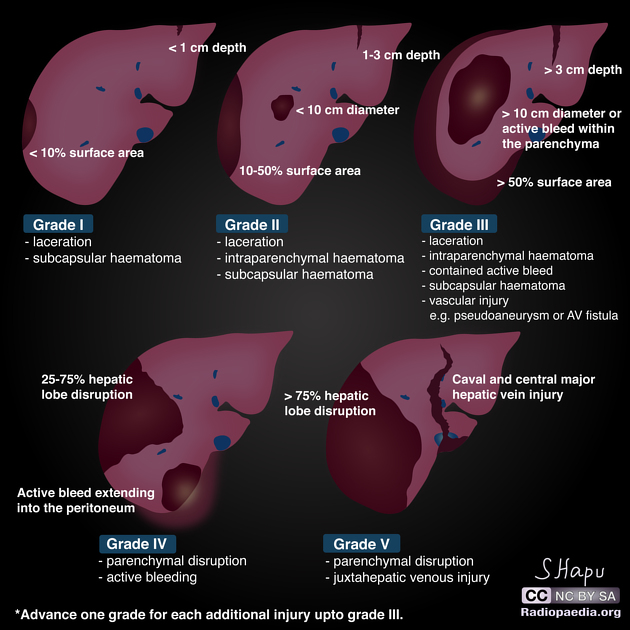
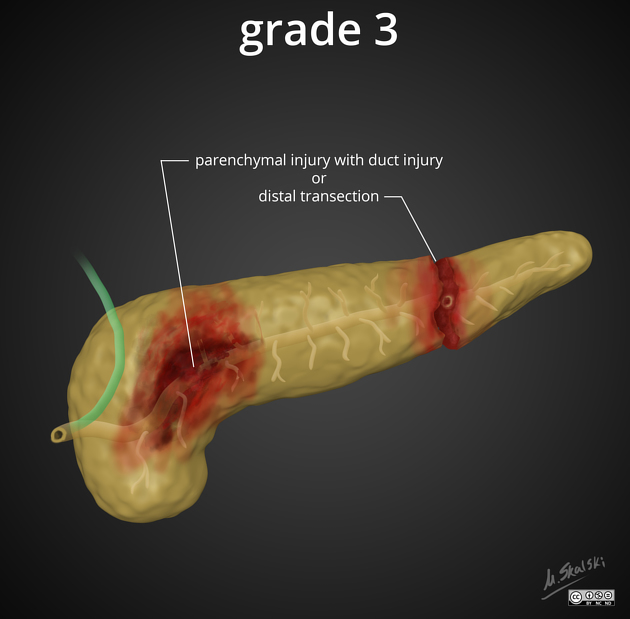
parenchymal organs: contusions, lacerations, devascularisation, parenchymal disruption or transection
hollow organs: contusions, lacerations with or without perforation, transection, devascularisation
vascular injury: irregularity or minimal injury, dissection, pseudoaneurysm, occlusion, transection
skin: incision, laceration, abrasion, puncture, penetration, contusion, avulsion, degloving
An overview of various traumatic injuries based on their location is given here 3-13:
-
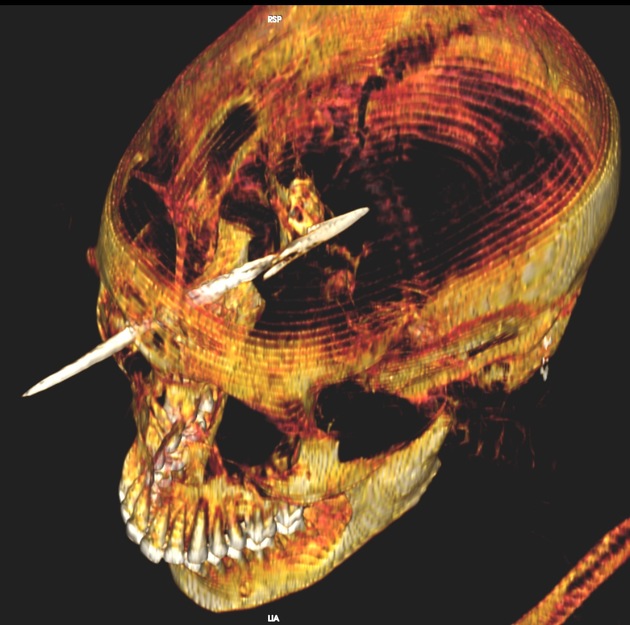
traumatic head injury
-
facial injury
injuries to the orbit and the eye
-
neck injuries
-
thoracic trauma
chest wall injury
-
lung injury
-
cardiac injury
penetrating cardiac injury
-
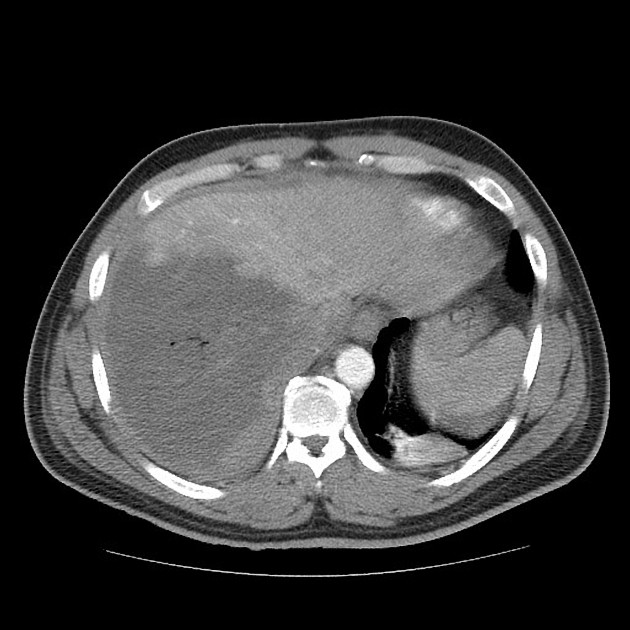
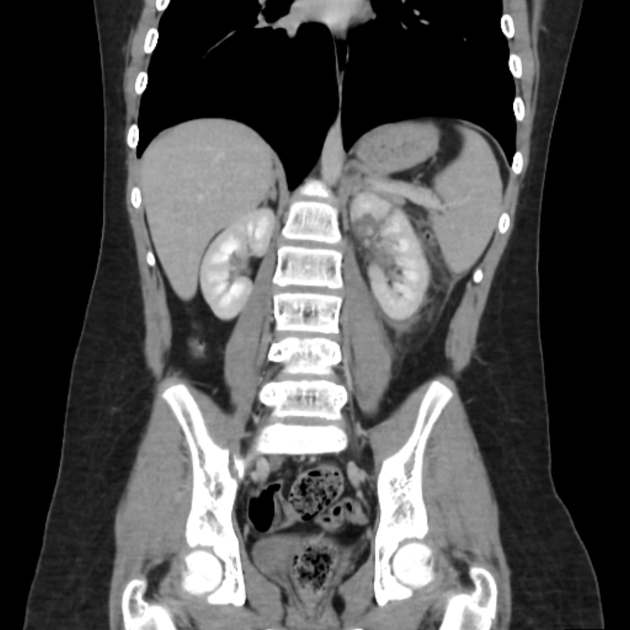
abdominal trauma
-
gastric injury
duodenal injury
small bowel injury
colon injury
rectal injury
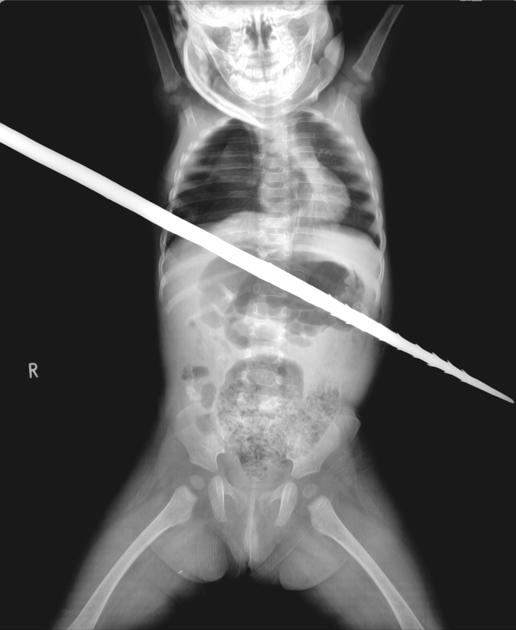
penetrating abdominal trauma
-
pelvic trauma
traumatic injury of the uterus
traumatic injuries of adnexa and/or ovaries
scrotal trauma
penile injury
-
spinal injuries
-
injuries to the extremities (most common)
-
injuries of the upper extremities
humeral fractures
radial and ulnar fractures
wrist injury and carpal fractures
injuries to the hand and fingers
-
injuries of the lower extremities
femoral fractures
tibial and fibular fractures
ankle injuries
midfoot and forefoot injuries
ligament and tendon injuries
peripheral vascular injuries
peripheral nerve injuries
traumatic limb amputation
-
Additional types of trauma or traumatic injuries include 2,7:
crush injury
burns
barotrauma
acoustic trauma
psychological trauma
Trauma scores
Trauma scores can be used to describe the extent of the whole injury such as the following:
Abbreviated Injury Scale (AIS): body region, anatomic structure and severity of the injury
Injury Severity Score (ISS): body region, injury severity
Radiographic features
Typical radiographic features of traumatic injuries include fractures, tears, contusions and lacerations in various degrees as well as the presence of haemorrhage or air in the soft tissues and outside the hollow organs.
Plain radiograph
Plain radiographs can nicely demonstrate and characterise fractures in the extremities and small joints 14. However, the diagnostic power in the detection of injuries in the trunk including the spine, thorax and pelvis is low as compared to MDCT 5,8.
Ultrasound
Ultrasound is widely and easily available and can be even used in the ambulance. A focused assessment with sonography for trauma (FAST) scan is particularly useful for the rapid detection of intra-abdominal and pericardial fluid 7-12 as well as the recognition of penetrating cardiac injuries. It is an important tool for assessing and triaging unstable patients in need of emergent surgery 5,7.
CT
CT is the gold standard and workhorse in the evaluation of severe and multiple traumatic injuries in haemodynamically stable or stabilised patients. It allows an effective detection and characterisation of life-threatening and unexpected injuries within a few minutes and can shorten hospital stay 5. In the setting of suspected polytrauma, it is usually acquired as a trauma-specific whole-body CT protocol 5. It has a crucial role in the evaluation of fractures and dislocations of the head and neck area, spine, chest wall and pelvis, and the assessment of the lungs 5. It is also a safe and accurate modality to evaluate deep-seated foreign bodies 7.
Non-contrast CT is required in the assessment of hyperacute traumatic brain injuries 5.
CT angiography allows for a fast and accurate evaluation of vascular injuries 5.
Contrast-enhanced CT is the modality of choice in the evaluation of traumatic abdominal organ injuries and the only radiographic modality for which dedicated organ injury scores within the diagnostic algorithm of traumatised patients exist 5,6, 8-12.
MRI
MRI can nicely depict the soft tissues, including the brain, the spinal cord, the muscles, tendons and ligaments, and the myocardium and the parenchyma of abdominal organs.
Due to the long acquisition times, MRI is rarely used in the hyperacute or acute setting and it might be even contraindicated in penetrating injuries, in which there is suspicion of retained metallic foreign bodies, e.g. shrapnel.
However, it plays an important role in the workup of spinal cord injuries as well as musculoskeletal injuries such as joints, muscles tendons and ligaments. It might be also indicated in specific brain injuries, pancreatic or bile duct injuries 5,12.
Further applications include a cardiac MRI in the setting of blunt cardiac injuries in haemodynamically stable patients or the parenchymal abdominal organs in patients and situations where radiation plays a major issue.
Angiography
Angiography might be performed in the setting of specific vascular injuries or for endovascular treatment of various injuries 8-11.
Radiology report
The radiological report should include the following:
type and extent of the traumatic injury
fracture classification
organ injury score
associated complications
Treatment and prognosis
Management and prognosis depend entirely on the type and extent of the specific injury and the complications associated with it 1.
Minor traumatic injuries might be seen and evaluated only clinically or might need further radiographic evaluation before definitive treatment.
Major traumatic events with multiple traumatic injuries will need immediate attention, care and possibly resuscitation on-site. Initial treatment follows the ABCDE rule and is focused on stabilising the patient 15. Once in hospital and stabilised, patients might get whole body polytrauma CT and further operative, non-operative or interventional treatment will be determined on the findings 16.
The initial radiographic evaluation of unstable patients might only include an ultrasound assessment before they directly go to the operating room for emergency surgery 17. However, those patients will most likely get further advanced support, intensive care and imaging after surgery 18 for a more comprehensive evaluation followed by further therapeutic and rehabilitative measures 1.
History and etymology
Trauma is directly taken from the Greek word τραυμα (trauma) meaning 'wound' and was first recorded in English in 1693 meaning a physical wound 21,24.















 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.