
Presentation
Left retro-orbital pressure pain and left-sided trigeminal nerve numbness with some diplopia.
Patient Data


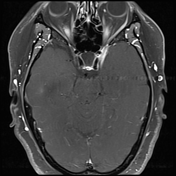
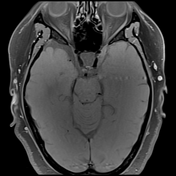
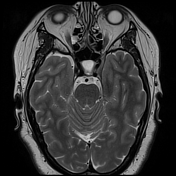
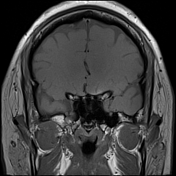
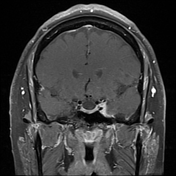
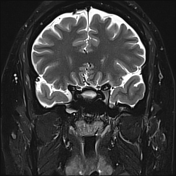
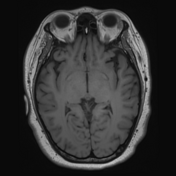
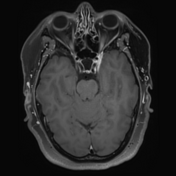
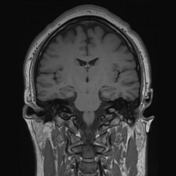
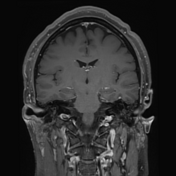
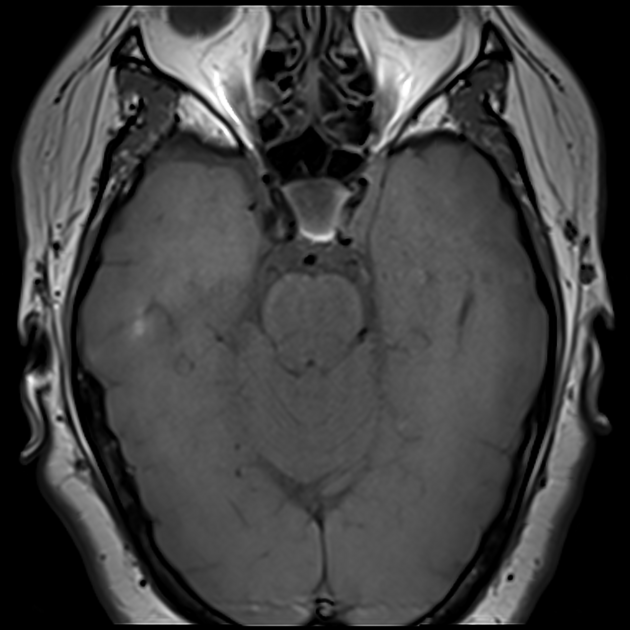
The lateral wall of the left cavernous sinus appears thickened and enhances vividly. It extends laterally involving Meckel's cave and surrounding the left trigeminal nerve with enhancement seen extending out of the skull through foramen ovale (along the mandibular division), foramen rotundum (maxillary division) and superior orbital fissure (ophthalmic division).
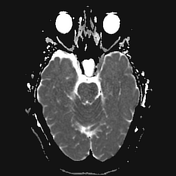
The left internal carotid artery is abutted by, and at least partially encircled by, enhancing tissue and maybe perhaps mildly narrowed. The pituitary fossa is mostly empty.
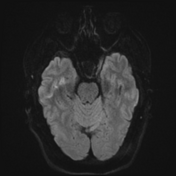
The remainder of the brain is unremarkable.
Case Discussion
The patient went on to have a lumbar puncture and lymph node biopsy.
Lumbar puncture
Cerebrospinal fluid: The smear contains a few lymphocytes as well as plasma cells and monocytes. No malignant cells are identified.
Lymph node biopsy
Right cervical lymph node core biopsy: The sections show lymph node parenchyma, skeletal muscle, fibroadipose tissue and some fibrinous material. The cell population is polymorphous, predominantly composed of lymphocytes, histiocytes and plasma cells. Germinal centers are not appreciable on H&E staining, however, there are scattered tingible body macrophages. There is no evidence of hyaline-vascular follicle change, mantle cell `onion skinning' or plasmacytosis. Eosinophils are not a feature. There is no sclerosis. No granulomas, atypical cells or necrosis are seen.
Immunohistochemistry highlights a mixed population of CD3+, CD5+ T-cells, CD20+, CD79a+ B-cells and CD68+ histiocyte population. CD21 and CD23 staining highlights one small dendritic cell meshwork associated with Bcl-6+ cells, consistent with a germinal center. There are scattered CD30+ immunoblasts. No atypical CD15, CD30 or PAX5 positive cells are seen. EBER-ISH shows scant positive small lymphocytes.
DIAGNOSIS: Non-specific reactive changes. There is no evidence of malignancy.
Treatment
The patient had a presumptive diagnosis of Tolosa-Hunt syndrome and was managed with steroids. There was little initial improvement and the treating clinicians were concerned that an alternative diagnosis existed (e.g. lymphoma, IgG4 disease, metastasis etc...)
The patient therefore underwent a cavernous sinus dural biopsy, which is usually not required in Tolosa-Hunt syndrome.
Cavernous sinus biopsy
Left cavernous sinus biopsy/lesion: The specimen consists of inflamed ganglion tissue and adjacent fibrous tissue with occasional small nests of meningothelial cells, SSTR2 positive on immunohistochemistry. Normal support cells are prominent around the ganglion cells. Immunohistochemistry highlights aggregates of reactive CD20-positive B cells and CD3-positive T cells. There is no nuclear atypia. Occasional plasma cells and rare neutrophils and eosinophils are admixed with the lymphocytes. There are no features of IgG4 disease on immunohistochemistry. Spirochete immunohistochemistry is negative.
DIAGNOSIS: Ganglion and fibrous tissue with mixed acute and chronic inflammation, and meningothelial hyperplasia. Consider infection and inflammatory causes.
Ongoing treatment
The findings remain consistent with a diagnosis of Tolosa-Hunt syndrome and the patient has made a good gradual recovery.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.