
Presentation
Intractable vertigo, lightheadedness, and dizziness for 4 days.
Patient Data


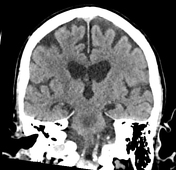
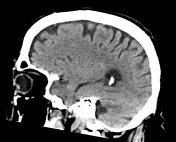
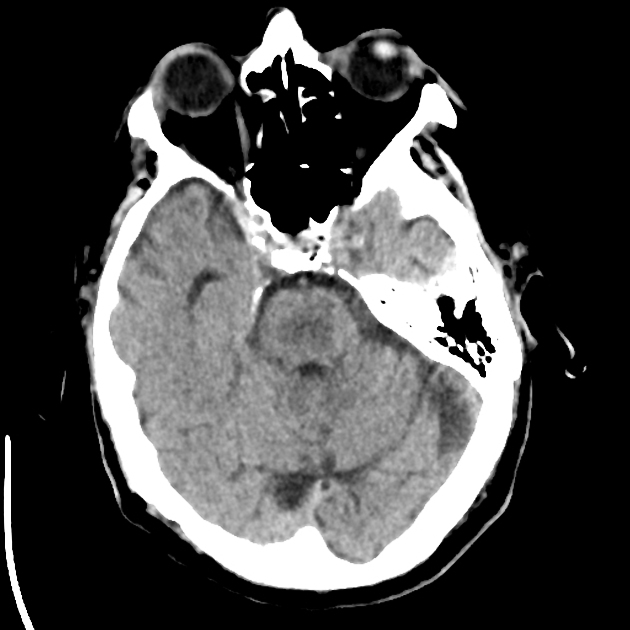
There is confluent low-attenuation in the central pons which is suspicious for central pontine myelinolysis/osmotic demyelination syndrome.

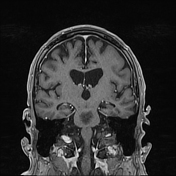
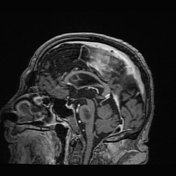
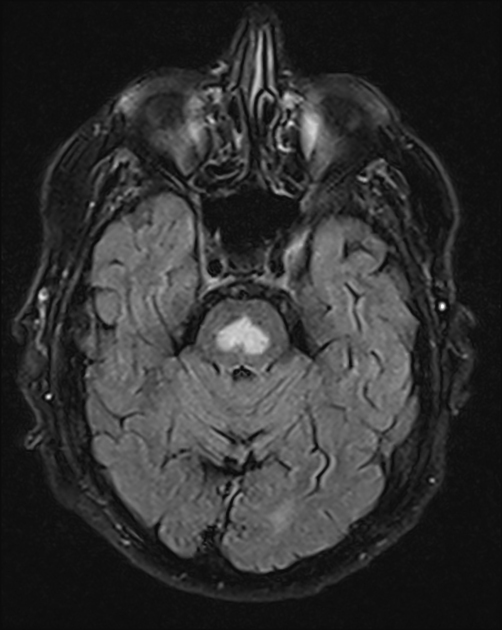
As noted on the CT study there is a large focus of non-enhancing T2 signal hyperintensity involving the central pons. This measures 1.9 x 1.2 cm in the axial plane and extends over a craniocaudal height of 1.8 cm. No associated restricted diffusion.
Impression:
Large focus of non-enhancing signal abnormality in the central pons, corresponding to low attenuation lesion on CT. The appearance is most suggestive of osmotic demyelinating syndrome (central pontine myelinolysis/CPM).
Case Discussion
This case most likely demonstrates osmotic demyelination syndrome (ODS), also known as central pontine myelinolysis (CPM). ODS is a serious neurological condition often associated with the rapid correction of severe hyponatremia. The patient presented with a serum sodium level of 120 mmol/L upon admission, which was rapidly corrected, likely contributing to the development of ODS.
ODS encompasses both central pontine myelinolysis and extrapontine myelinolysis, characterized by demyelination in the central pons and other brain regions. The pathophysiology involves osmotic stress leading to cerebral apoptosis and myelin loss, particularly in areas rich in oligodendrocytes and myelin 7. Rapid correction of hyponatremia is a well-documented risk factor for ODS, with the American Association for the Study of Liver Diseases recommending a controlled rate of sodium correction to mitigate this risk.
Magnetic resonance imaging (MRI) remains the gold standard for diagnosing ODS, as it is superior to non-contrast computed tomography (CT) in detecting the characteristic lesions. MRI findings typically include hyperintense lesions on T2-weighted and fluid-attenuated inversion recovery (FLAIR) sequences in the pons and other affected areas 8. Diffusion-weighted imaging (DWI) can detect early changes within 24 hours of symptom onset, which are not visible on conventional MRI sequences 9 .
The clinical presentation of ODS can be biphasic, initially reflecting the underlying condition (e.g. hyponatremia) followed by neurological deterioration, including symptoms such as dysarthria, dysphagia, oculomotor dysfunction, and quadriparesis. In this case, the rapid correction of hyponatremia likely precipitated the development of ODS, as evidenced by the patient's clinical deterioration and MRI findings.
In conclusion, this case underscores the importance of cautious correction of hyponatremia to prevent ODS. MRI is essential for early and accurate diagnosis, allowing for timely intervention and management. Despite advances in diagnostic techniques, ODS remains a critical condition with significant morbidity and mortality risks.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.