
Presentation
Pain in the left proximal posterior thigh and discomfort in the buttocks. Clinical suspicion for a hamstring injury.
Patient Data


Findings
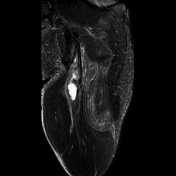
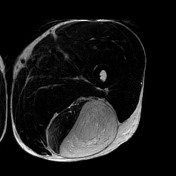
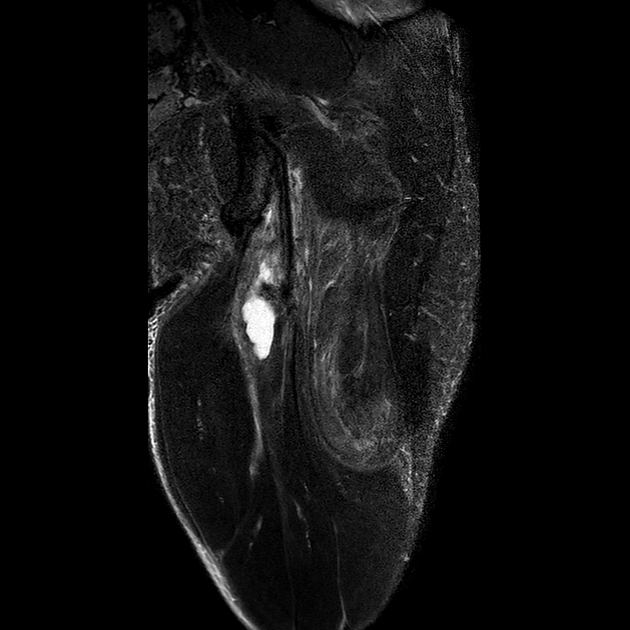
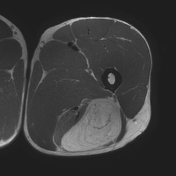
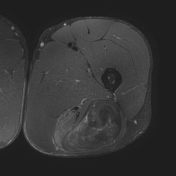
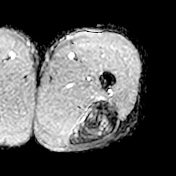
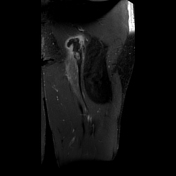
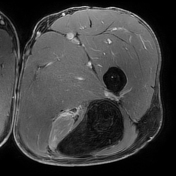
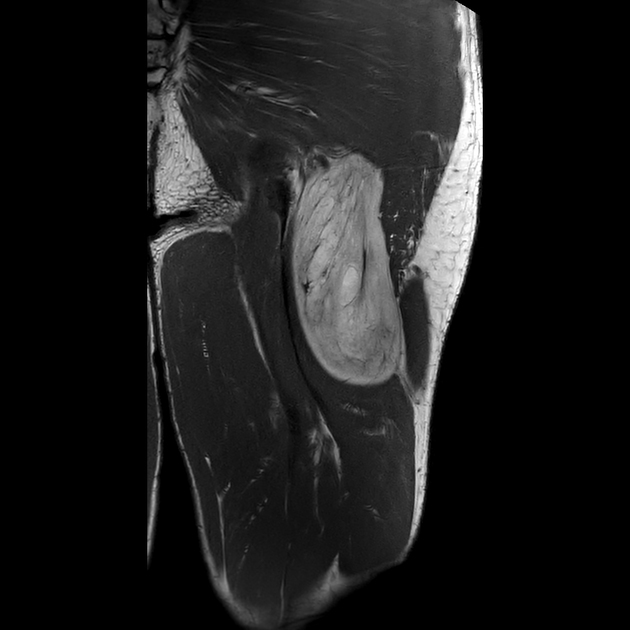
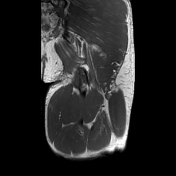
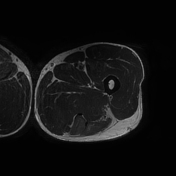
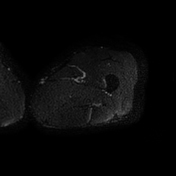
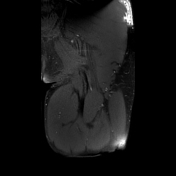
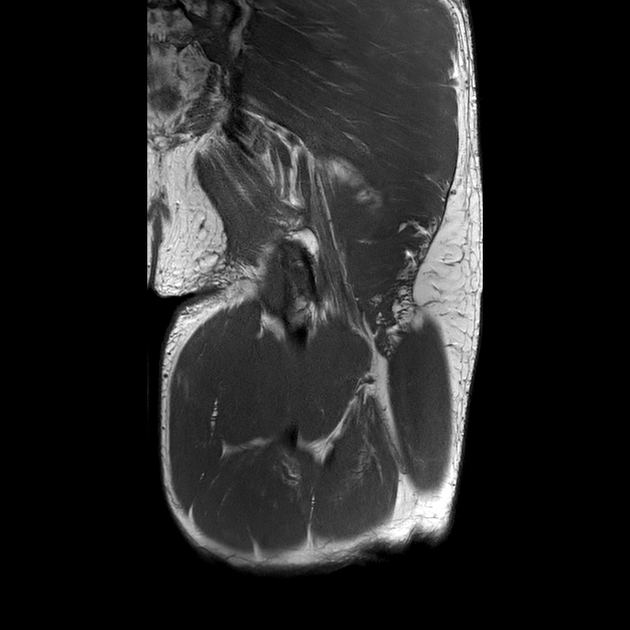
fluid-filled gap at the proximal insertion site of the hamstring muscles between the conjoint tendon and the proximal semimembranosus tendon extending further distally into the myotendinous junction
avulsion of the conjoint semitendinosus and biceps femoris tendon with >2cm retraction
partial tear of the semimembranosus tendon insertion
proximal muscle edema but no atrophy or fatty degeneration of the semitendinosus and biceps femoris longus muscles
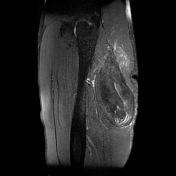
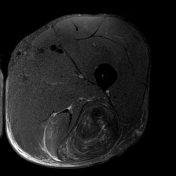
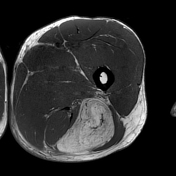
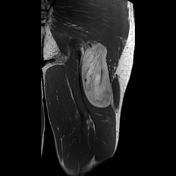
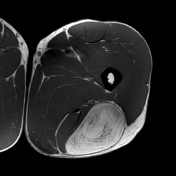
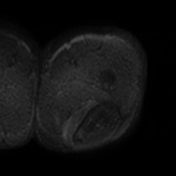
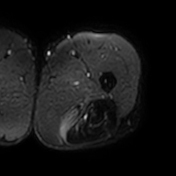
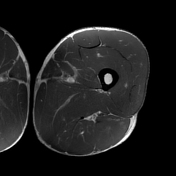
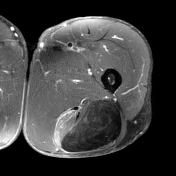
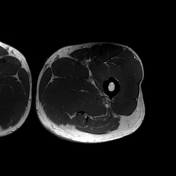
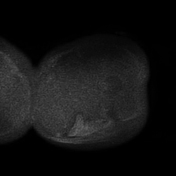
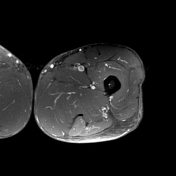
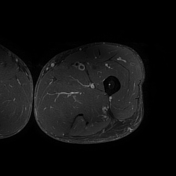
large lipomatous tumor in a subfascial location lateral to the biceps femoris muscle and proximally underneath the caudal portion of the gluteus maximus muscle
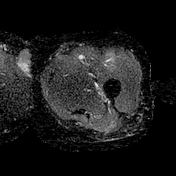
predominantly thin septae, two septae with a borderline thickness of ~2 mm in the mid-caudal and medial portion of the tumor
some septae show an increased signal on fluid-sensitive images
tumor dimensions: ~17 x 9.5 x 6 cm
the course of the sciatic nerve in a close relationship, lateral to the avulsed conjoint tendon and medial to the lipomatous tumor
Impression
proximal hamstring injury with a full-thickness tear of the conjoint tendon (>2 cm tendon retraction) and partial tear of the proximal semimembranosus tendon
incidental large subfascial lipomatous tumor in keeping with either a large intermuscular lipoma or atypical lipomatous tumor
Exam courtesy: Jeanette Moses (imaging technologist)
Findings
lipomatous tumor
no focal nodular patchy non-fatty tissue components of the tumor
no thick or nodular contrast enhancement of the septae
phase-encoded motion artifact in the lower portion of the tumor in the fat-saturated T1 C+ sequence not reproduced in the Dixon C+ sequence
no diffusion restriction, blackout effect
proximal hamstring injury
thick reactive enhancing fibrovascular tissue around the proximal hamstring tear
Impression
large lipomatous tumor - intermuscular lipoma favored over an atypical lipomatous tumor
due to the large size histology was recommended
known proximal hamstring injury
Exam courtesy: Torsten Otte (imaging technologist)
The patient underwent surgical resection of the tumor.
Pathology report (translation)
Macroscopic appearance
- encapsulated, nodular, soft-elastic piece of tissue
- dimensions: 14.5 x 2.5 x 7 cm
- cut surface: yellowish lobulated soft-elastic tissue
Microscopic appearance
- soft tissue extirpate of mature lobulated adipose tissue, delicately encapsulated and the fat lobules interspersed with connective tissue
- adipocytes with similar sizes and without nuclear atypia
- no hemorrhage or necrosis
Diagnosis
- benign subfascial lipoma of the thigh

Findings
status post tumor resection.
no evidence of contrast-enhancing lesions, no residual lipomatous mass
known old proximal hamstring injury with a full-thickness tear of the conjoint semitendinosus and biceps femoris tendons
slight edematous changes of the semitendinosus muscle and biceps femoris muscle
no atrophy or fatty degeneration
sciatic nerve inconspicuous
Impression
after tumor resection, no tumor remnant
known old proximal hamstring injury with avulsion of the conjoint tendon
normal-appearing sciatic nerve
Exam courtesy: Ines Lischka (imaging technologist)
Case Discussion
A case of a proximal hamstring injury with avulsion of the conjoint tendon and a large incidentally found intermuscular lipoma.
Differentiating large intermuscular or intramuscular lipomas from atypical lipomatous tumors might be challenging in imaging. The following criteria favor lipoma vs atypical lipomatous tumor 1-4:
no focal nodular patchy non-fatty tumor components
predominantly thin, non-enhancing septae
The large tumor size >13 cm made the decision more difficult favoring the diagnosis of an atypical lipomatous tumor on MRI 1-4. The few septae with borderline thickness and the foci or regions of increased signal intensity on fluid-sensitive images did not help in the decision 1-4.
Eventually, the tumor was resected and histology revealed subfascial lipoma (see above).
MRI can aid in guiding management decisions of proximal insertional injuries 4-6 of the hamstring muscles with respect to the tear type (partial thickness/full-thickness), the tendon retraction and the tendons involved. Surgical treatment should be considered in complete hamstring avulsion with retraction of both the conjoint and semimembranosus tendon whereas partial thickness tears and full-thickness tears with tendon retraction are often treated non-operatively and retracted single tendon tears might be treated with respect to chronicity and patients wishes and needs 4-6. In this case, the insertional tear was not repaired surgically.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.