
Presentation
Seizures.
Patient Data


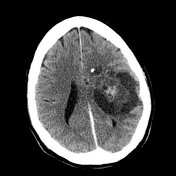

A large mass consisting of a solid central component and a cystic peripheral component exerts localized mass effect on the left hemisphere. Anteriorly a number of heavily calcified components are also present.
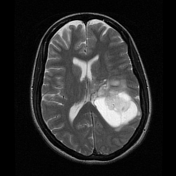

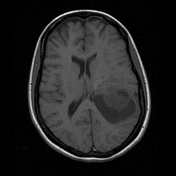
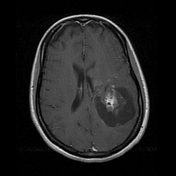
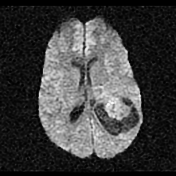
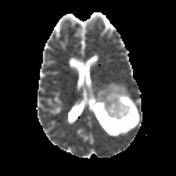
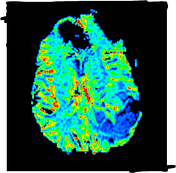
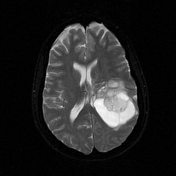
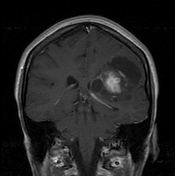
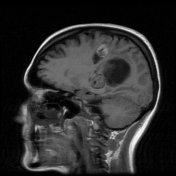
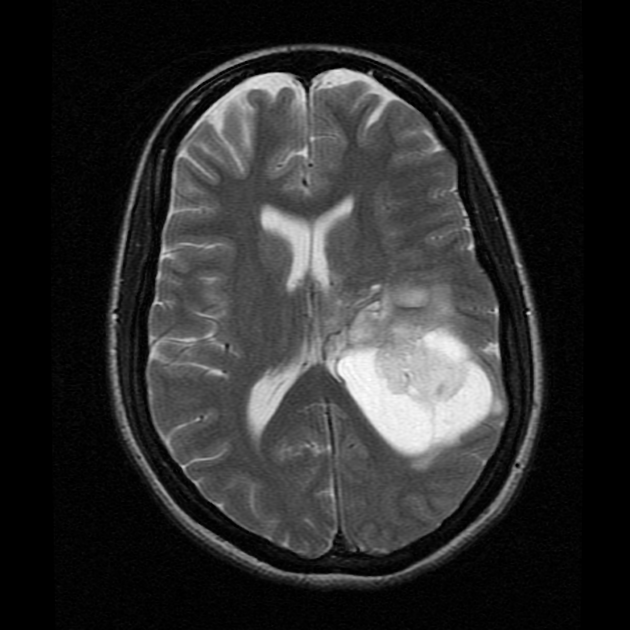
A large solid and cystic mass centered on the posterior left frontal lobe and frontoparietal junction has broad contact with the ependymal surface of the left lateral ventricle with minimal surrounding edema. A focus of signal loss (on T2 weighted scans) at the anterosuperior aspect of the mass correlates with the largest focus of calcification visible on CT. There is moderate patchy enhancement of the solid components. This solid region demonstrates fairly high cerebral blood volume similar to that of cortex. ADC values are facilitated compared to the surrounding brain. Spectroscopy shows mildly elevated choline, elevated myo-inositol and decreased NAA (not shown).
The temporal horn of the left lateral ventricle is dilated related to compression by the dominant cystic component, but there is no ventricular dilatation elsewhere.
Conclusion
Large solid and cystic neoplasm centered on the posterior left frontal lobe and frontoparietal junction. Cortical involvement, coarse calcification and subependymal spread are evident. Of the broad differential, oligodendroglioma (grade 2 or possibly 3) and ganglioglioma are considered the most likely. Less likely possibilities include pleomorphic xanthoastrocytoma and DNET.
The patient went on to have a resection.
Histology
Paraffin sections show a moderately cellular glioneuronal tumor. There are loose clusters and sheets of atypical astrocytes showing nuclear enlargement, nuclear pleomorphism and hyperchromatism. Many areas show microcystic degeneration in the background. Minor component of stromal fibrosis is also identified. Haphazardly scattered within the astrocytic component are atypical unoriented ganglion cells, showing cytomegaly and dysmorphism. Many eosinophilic granular bodies and occasional Rosenthal fibers are also identified. Many scattered lymphocytes are present within the tumor as well as cuffing the tumor vessels. Occasional scattered mitoses are seen. There is no necrosis or microvascular proliferation.
The astrocytic component shows strong positivity for GFAP. The atypical ganglion cells show strong staining for synaptophysin and Beta-tubulin. Some of the ganglion cells show weak staining for NFP and there is negative staining for Neu-N. The IDH-1 stain is negative. The Ki-67 proliferative index is approximately 1%.
Final diagnosis
Low-grade glioneuronal tumor favoring a ganglioglioma (WHO Grade I).
Case Discussion
This is a good example of a ganglioglioma, although typically they are located in the temporal lobes.
This patient was lost to follow-up. Repeat imaging 5 years later showed slow-growing recurrent/residual nodules.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.