
Presentation
Abdominal pain, nausea and vomiting. History of laparotomy 20 years ago.
Patient Data



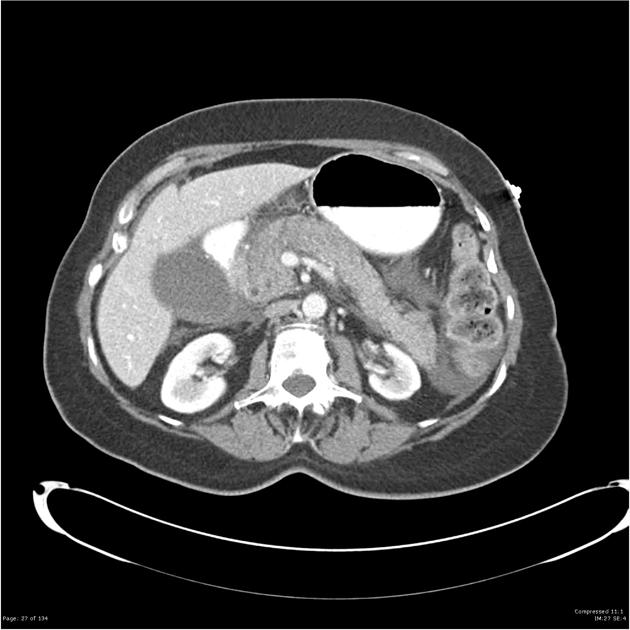
Peripancreatic inflammatory fat stranding as well as a moderate volume of retroperitoneal free fluid. A small amount of mesenteric and perihepatic fluid is also demonstrated. The gallbladder is distended, with multiple radiopaque gallstones. No pancreatic lesion is detected. No evidence of pancreatic necrosis. The common bile duct is visualized and does not appear to be dilated. No intrahepatic bile duct dilatation. No evidence of a pseudoaneurysm, splenic or portal vein thrombosis. The liver, spleen, adrenals and right kidney are within normal limits. The left kidney is atrophic, with evidence of cortical scarring. No hydronephrosis. Apart from colonic fecal loading, the bowel is unremarkable. No pneumoperitoneum.
Case Discussion
Features are typical of acute pancreatitis, secondary presumably to gallstones.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.