
Presentation
Wrist pain. Trauma 5 years ago.
Patient Data


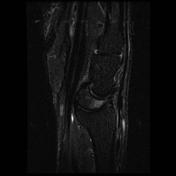
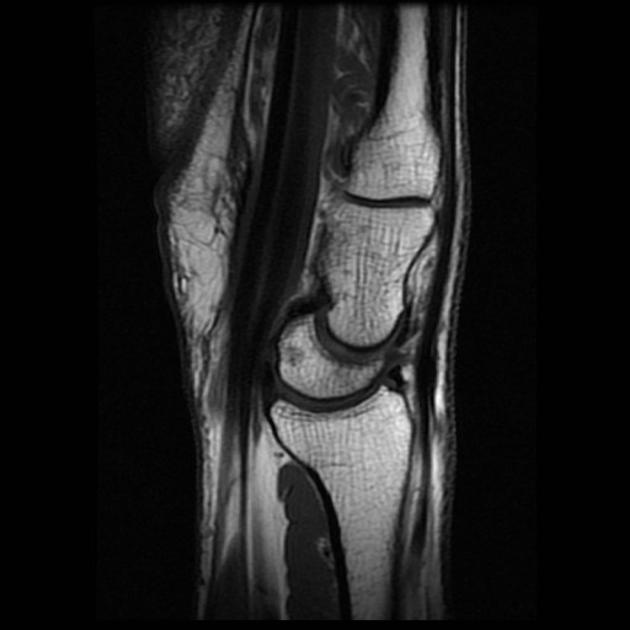
MRI shows subtle edema involving the dorsal aspect of the lunate. Moreover, there is slight posterior displacement of the capitate compared to the distal radius, the luno-capitate angle is > 30°. The lunate is displaced dorsally (the anterior apex of the lunate points more dorsally). Harder to measure on MRI, the scapholunate is also greater than 60°.
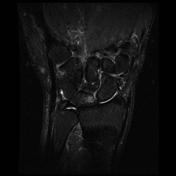
Moreover, there is a slight increase in the scapholunate distance dorsally, near the lunate contusion, compatible with scapholunate ligament tear.
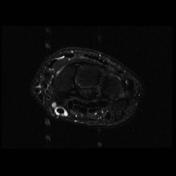
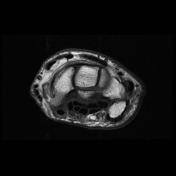
This patient also has a flexor carpi radialis tenosynovitis.


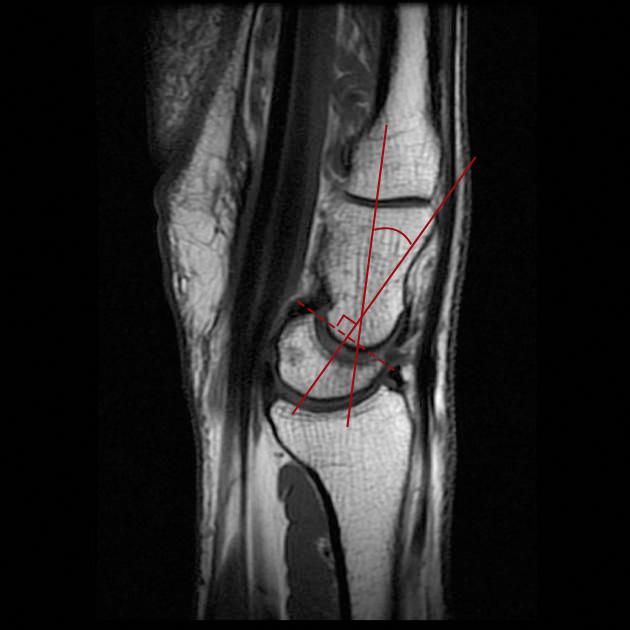
This diagram shows how to draw the capitolunate angle which should be less than 30 degrees, and scahpolunate angle (which is generally drawn on plain film) which should be less than 60 degrees.
The axis of the lunate is drawn as a perpendicular to a line connecting the to poles for both measurements.
A line is drawn along the axis of the capitate, through the apex of the proximal artiular surface as a best fit line for the capitolunate angle.
A tangent is drawn along the volar surface of the scaphoid for the scapholunate angle.
Case Discussion
This case shows the usual manifestations of DISI. It is harder to appreciate on MRI since the scapholunate and capitolunate angles are harder to measure with precision.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.