
Presentation
Rapid onset upper and lower limb symptoms.
Patient Data




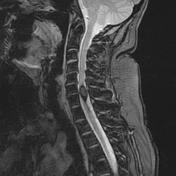
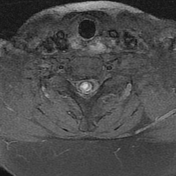
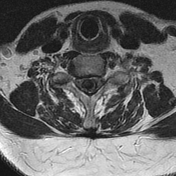

MRI of the spine demonstrates an intramedullary lesion which intrinsic high T1 signal and no convincing enhancement. It is surrounded by very low signal on T2 weighted images, which demonstrates blooming on gradient echo.


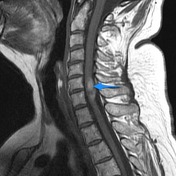


Complete hemosiderin ring (red arrow) demonstrates blooming on gradient echo sequences (yellow arrow). Intrinsic high T1 signal (blue arrow) is visible on both pre and post contrast sequences and should bot be mistaken for contrast enhancement.
MICROSCOPIC DESCRIPTION: The section shows a nidus of large and small caliber vascular channels. No elastic tissue is identified in the walls of these vessels. The lumen of one of the large vessels is filled with blood clot.
FINAL DIAGNOSIS: Features suggestive of vascular malformation; no evidence of tumor seen.
Case Discussion
It is always important to remember that not all spinal cord masses are tumors, and that lesions which would be simple to diagnose in the brain, can mimic spinal cord tumors. The absence of any enhancement and the complete peripheral hemosiderin ring are helpful in this case.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.