
Presentation
Presented with lower limb weakness. Had a non-diagnostic biopsy (sample too small) months earlier. Now progressive symptoms.
Patient Data




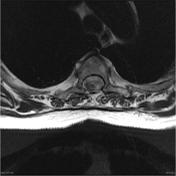



Previous T1 to T4 laminectomy. A mass lesion measuring approximately 2 2 x 0.7 x 0.5 centimeters lies at the posterior and right side of the cord at the T2/T3 level. It is associated with expansion of the cord and extensive edema that extends from the C7 level down to the inferior limits of the scan.
The sagittal images suggests an intra-medullary location. The axial images suggest an exophytic component posteriorly. The mass is iso-intense to hypointense to cord on T1 and markedly hypointense on T2 weighted images. The hypointense component is associated with a marked contrast enhancement. No other areas of abnormal contrast enhancement are seen.


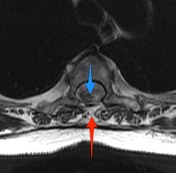
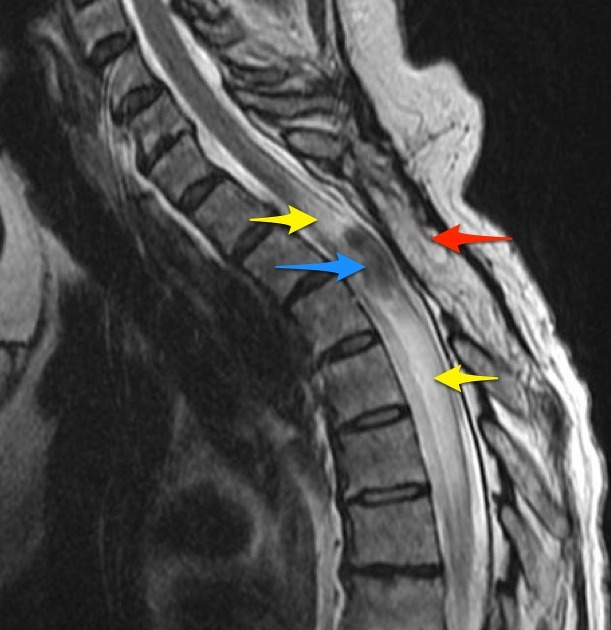
The tumor (blue arrows) is of low signal on T2 and T1 sequences and demonstrates vivid contrast enhancement. It is associated with rostral and caudal edema (yellow arrows). Previous laminectomy (red arrows) is visible.
Histology
MACROSCOPIC DESCRIPTION: Spinal cord tumor: A piece of rubbery pink to fawn tissue 20x5x6mm.
MICROSCOPIC DESCRIPTION: The sections show a well-demarcated tumor with hyper and hypocellular areas. In the cellular areas, the tumor forms short fascicles. The tumor cells have elongated nuclei, hyperchromasia and scanty ill-defined cytoplasm. 1 mitosis per 10 high power fields is seen. Some staghorn type blood vessels are present in the background, which is focally fibrosed, containing keloidal-type collagen bundles. No necrosis is identified. The tumor cells are CD34 and CD99 positive. Factor XIIIa is focally and weakly positive. They are EMA, AE1/3, S-100 and Melan-A negative. The Ki-67 index is about 4%. The features are in keeping with a solitary fibrous tumor.
FINAL DIAGNOSIS: Spinal cord tumor: Solitary fibrous tumor of the spinal cord.
Case Discussion
Though most solitary fibrous tumors are benign, some may behave aggressively and long term follow-up is mandatory. There are no features of malignancy in this biopsy (namely moderate to marked cytological atypia, tumor necrosis, more than 4 mitoses per 10HPFs, infiltrative margins).


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.