
Presentation
Abdominal pain
Patient Data


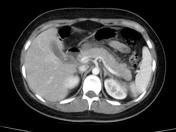



Pancreatic swelling and peripancreatic stranding, extending to the left pararenal space (thickened Gerota's fascia). The pancreas is enhancing homogeneously, with no signs of necrosis on CT. No pancreatic duct dilatation.
The gallbladder is suboptimally seen, but there is suspicion of stone in its neck. A gallbladder ultrasound scan is suggested. No evidence of biliary dilatation.
No evidence of walled-off collection.
Portal, splenic, and SMV are opacified normally. No evidence of splenic artery pseudoaneurysm.
Minimal left-sided pleural effusion and associated basal atelectasis.
Interpretation: Features of acute pancreatitis.
Case Discussion
This case shows an acute pancreatitis with peripancreatic edema, inflammation without pancreatic necrosis and abnormal peripancreatic fat, probably secondary to a biliary pathology.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.