
Presentation
Abdominal pain
Patient Data
Age: 17 years
Gender: Female



Download
Info
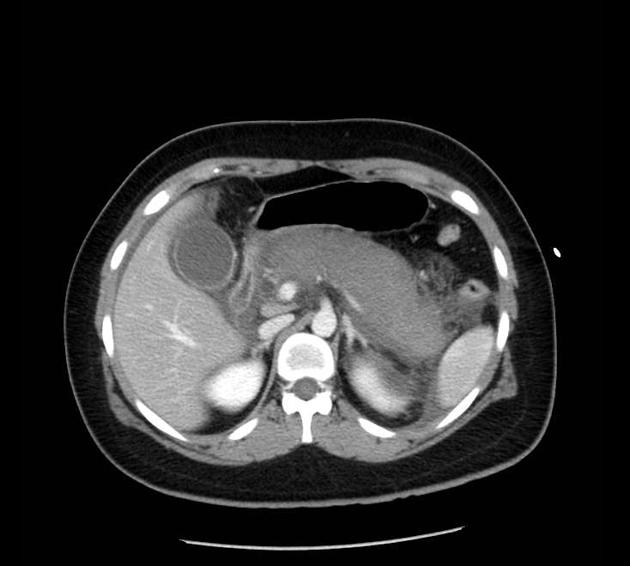
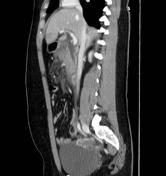
The pancreas is swollen and the majority of the parenchyma is non-enhancing. Only a small amount of normally enhancing parenchyma is seen in the region of the pancreatic head. It displayed a marked dilatation of the common bile duct
Case Discussion
CT reveals non-enhancement of pancreatic body and tail, indicating pancreatic necrosis.
The chief role of CT imaging in acute pancreatitis is to look for complications and hence imaging advised 48-72 hours after presentation. If the clinical information permits, a multi-phase pancreatic study is recommended to best illustrate necrosis, in addition to other potential complications, such as peri-pancreatic collection, abscess, and pseudoaneurysm.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.