
Presentation
Lower abdominal pain for 5 days with associated nausea, anorexia and constipation. Suprapubic tenderness on examination.
Patient Data
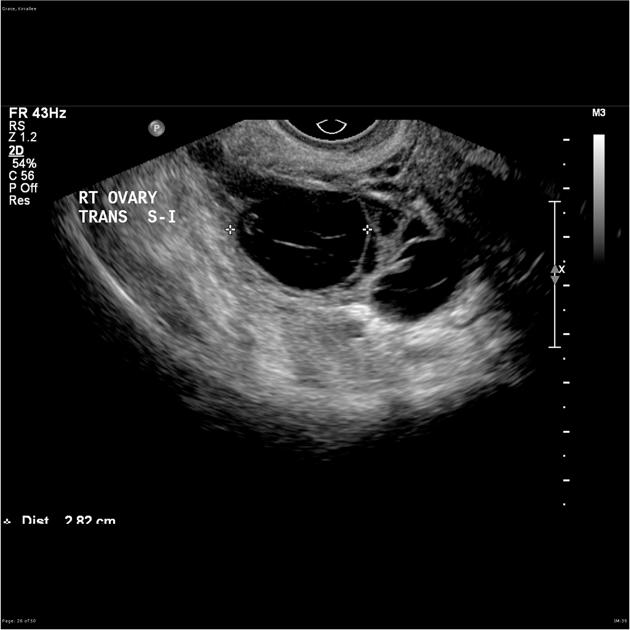
Transabdominal and transvaginal pelvic ultrasound images showing a normal appearing anteverted, anti-flexed uterus. Endometrial stripe measures 4mm. Both ovaries are identified. The left ovary has a normal appearance. The right adnexae contains a complex, predominantly cystic mass which has an US appearance most in keeping with a tubo-ovarian abscess. An ectopic pregnancy can not be completely excluded. There is a small amount of free pelvic fluid identified.
Insinuation of the complex mass into anatomical spaces is more in keeping with a tubo-ovarian abscess. No fetal parts to support an ectopic preganancy but could not entirely exclude an cystic ovarian mass.
Acknowledgement: Prof Brian Tress.
Case Discussion
An interesting case highlighting the difficulty in differential diagnosis between a tubo-ovarian abscess, cystic ovarian tumor, and ectopic pregnancy. Whilst likely showing a right tubo-ovarian abscess, in the clinical context a cystic ovarian tumor is considered less likely and an ectopic pregnancy cannot be excluded. Correlation of imaging findings with the beta HCG was recommended in discussions with the treating clinician.
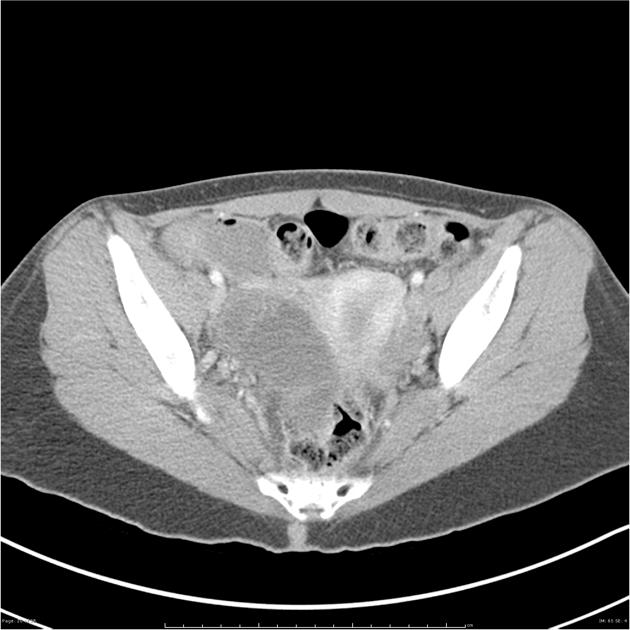
A CT abdo/pelvis with contrast 6 days later showed insinuation of the complex mass into anatomical spaces more in keeping with a tubo-ovarian abscess, did not show any fetal parts to support an ectopic pregnancy but could not entirely exclude a cystic ovarian neoplasm.
A repeat US 1 month later found the cystic mass within the right adnexa to have increased in size with ultrasound appearance in keeping with hydrosalpinx or tubo ovarian abscess.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.