
Presentation
Diffuse abdominal pain.
Patient Data
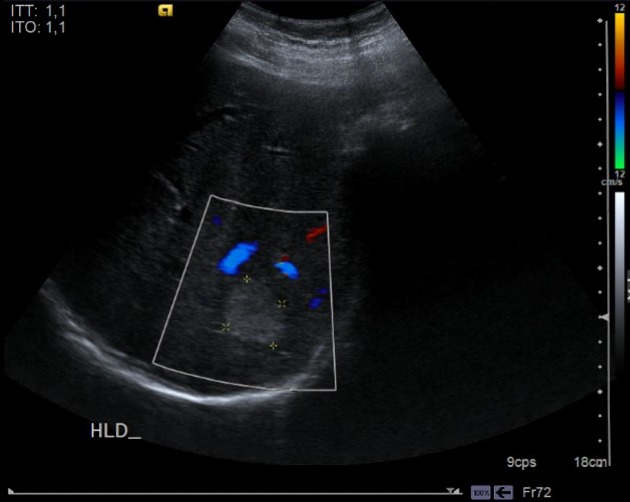
Abdo US performed few hours after come to the emergency room
Liver with normal echostructure and morphology. In the posterior segment of the right hepatic lobe of a homogeneous hyperechogenic 2.9 x 2.5 cm focal lesion is seen, without demonstrable vascular flow with doppler study. Gallbladder not displayed (surgical history).
Intrahepatic Biliary tract caliber preserved. The extrahepatic biliar duct reaches 8 mm at the common hepatic duct, common to observe in cholecystectomy patients finding. Obstructive cause is not observed in this study.
Spleen and pancreas normal.
Both kidneys are of normal size and morphology. Exhibit adequate cortical thickness and good differentiation between parenchyma and renal sinus. No pielocaliciaria dilation or suggestive images of calculations. Visible path of the abdominal aorta preserved caliber.
No intraabdominal free fluid is identified.
After persisting pain, decided to perform MRI.
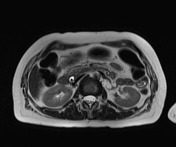

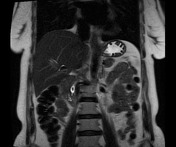



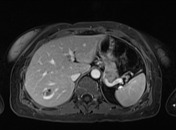

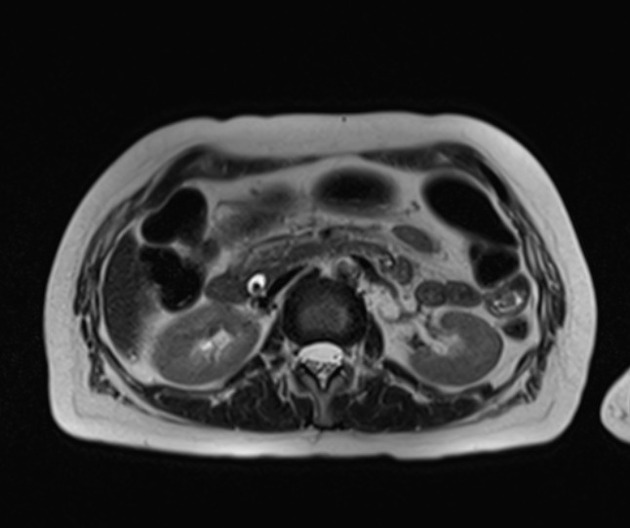
Liver of size, morphology and signal are normal. In the posterior segment (VII) hemangioma 2.5 cm is observed. No aggressive focal lesions observed in the thickness of the parenchyma.
Main portal vein and its intrahepatic branches, splenic-mesenteric venous system and hepatic veins permeable. Postsurgical changes cholecystectomy. Cystic duct remnant normal signal. Mild dilatation of the intrahepatic central bile duct. The extrahepatic biliar duct reaches 7 mm at the common hepatic duct. At the level of the distal common bile intrapancreatic hypointense filling defect is observed, lying dependently, consistent with an gallstone estimate of 7 mm. Papillary segment free at the time of examination.
It was decided to perform ERCP, 7 days after the patient has deteriorating condition, highlighting elevated pancreatic enzymes. Computed tomography of the abdomen and pelvis is indicated for possible complications
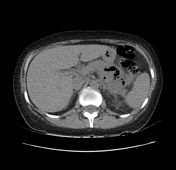



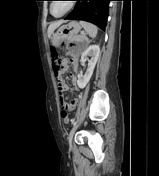

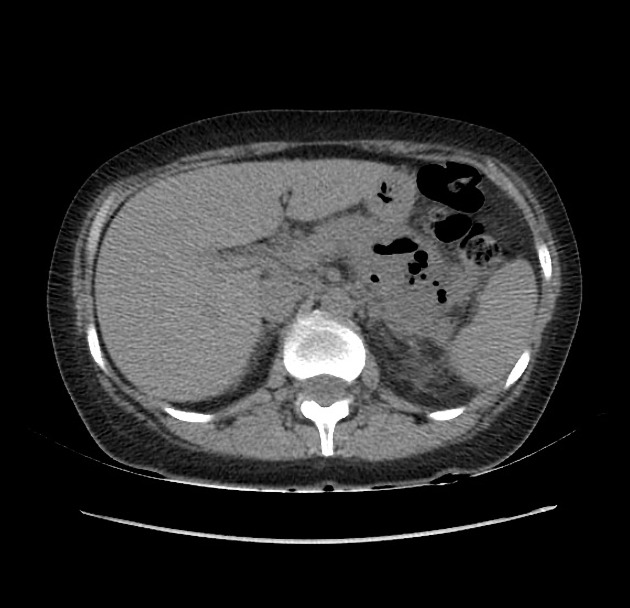
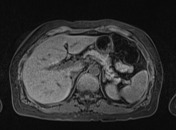
Liver size and normal morphology. In the posterior segment of the right hepatic lobe a image is observed with peripheral,nodular inturrupted enhancement with vascular pattern pool, 2.5 cm long axis, consistent with a cavernous hemangioma.
In relation to the tail of the pancreas a collection of approximately 6.6 cm at the widest point of which has defined walls and some gas bubbles in appearance not dependent changes associated with certain inflammatory adipose tissue immediately adjacent the pancreatic parenchyma. No alterations are observed in the pattern of impregnation with the use of intravenous contrast medium.
Case Discussion
Findings consistent with acute pancreatitis Balthazar E. This case demonstrates a subsequent ERCP-induced pancreatitis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.