
Presentation
1 week history of bilateral parotid swelling. Background of Sjogren's disease
Patient Data
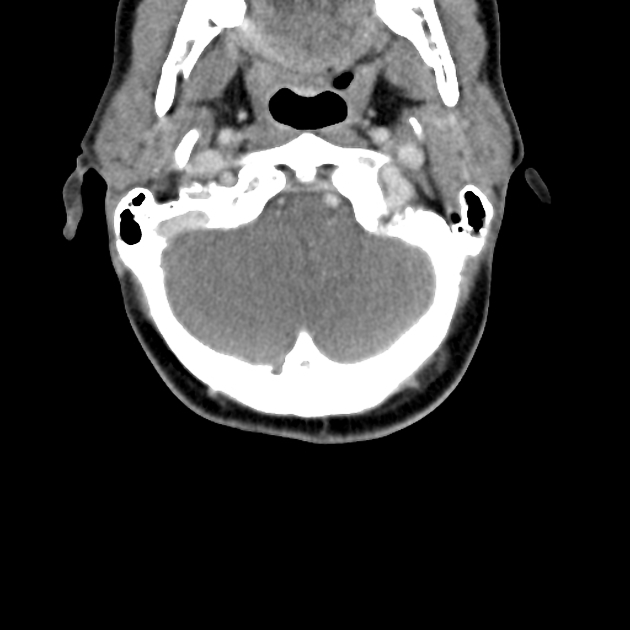
Both parotid glands are heterogenous with cystic regions consistent with the intermediate stage of Sjogren's disease. The submandibular glands are atrophic. No calcification identified within the parotid or submandibular glands.
There is diffuse enlargement of multiple lymph nodes within the neck. There is a level 1 lymph node measuring 2 cm. Enlarged left level 2/3 nodes measuring up to 2.5 cm. Enlarged right level 3 nodes measuring 2.5 cm.
The extent of lymphadenopathy extends into the down upper chest, with multiple small left infraclavicular nodes identified.
The pharynx and larynx have a normal appearance. The thyroid gland is unremarkable.
Conclusion:
- salivary gland changes are consistent with Sjogrens syndrome
- extensive lymph node enlargement within the and neck and axilla. Splenomegaly. This is suggestive of lymphomatous transformation
- the neck or left axillary lymph node would be amenable to ultrasound-guided biopsy
There is a left axillary node measuring 2.4 cm in long axis. Multiple enlarged right axillary lymph nodes. No convincing lymphadenopathy identified within the mediastinum.
Note is made of a retro esophageal course of the right subclavian artery with mild mass effect upon the esophagus.
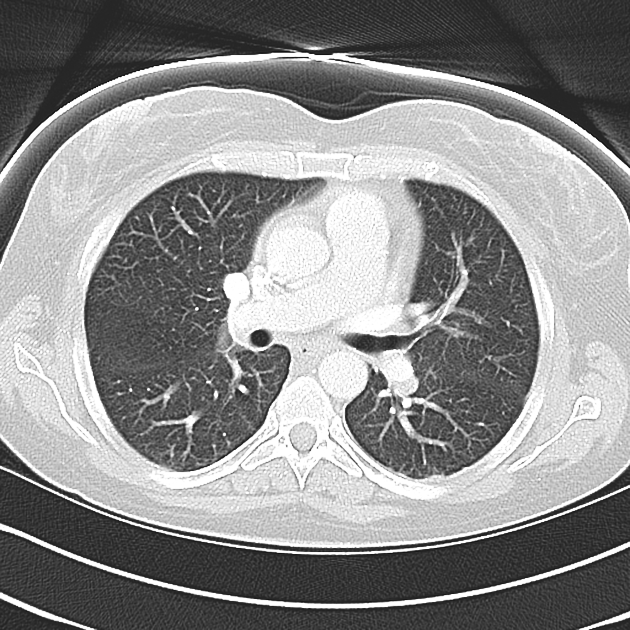
There is collapse with loss of volume seen at the left lower lobe. Some of the collapsed lung demonstrates heterogeneous enhancement. There is a small left-sided pleural effusion. Atelectasis at the right lung base. Subpleural nodule associated with the minor fissure.
There are two lung cysts seen within the posterior aspect of the right upper lobe potentially related to previous infection - with lymphocytic interstitial pneumonitis thought less likely though not excluded given the immunological predisposition.The central airways are unremarkable.
No pericardial effusion.
Review of the imaged upper solid organs demonstrates an enlarged spleen with multiple peripheral regions of low density. The likely etiology is multiple splenic infarcts.
Conclusion:
The changes at the left lung base may be sympathetic related to the subdiaphragmatic splenic infarcts with superimposed infection not excluded.
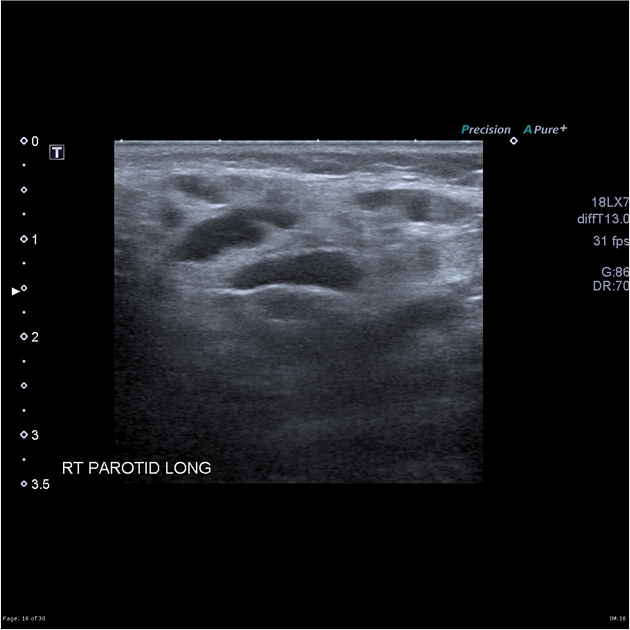
Both parotids and both submandibular glands are enlarged with multiple small cystic foci which do not appear contiguous with a duct, though the duct itself could not be seen. There are enlarged lymph nodes within both parotid glands. No calcifications are evident.
Conclusion:
Changes in the parotid and submandibular glands bilaterally are in keeping with the intermediate stage of Sjogren involvement.
Case Discussion
Key points:
1. the cystic change is often better appreciated on ultrasound
2. cysts in the submandibular glands suggest Sjogren's disease rather than HIV
3. Sjogren's disease is associated with lymphoma


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.