
Presentation
Renal transplant patient with progressive bulbar symptoms.
Patient Data
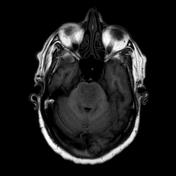


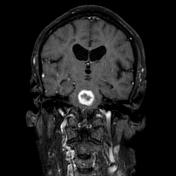
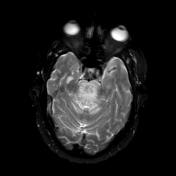
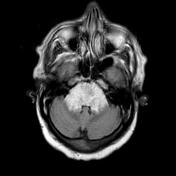
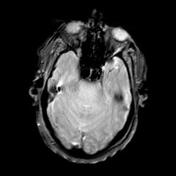
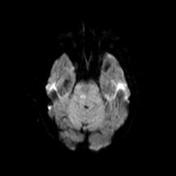
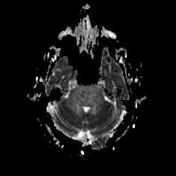


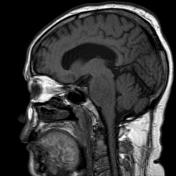
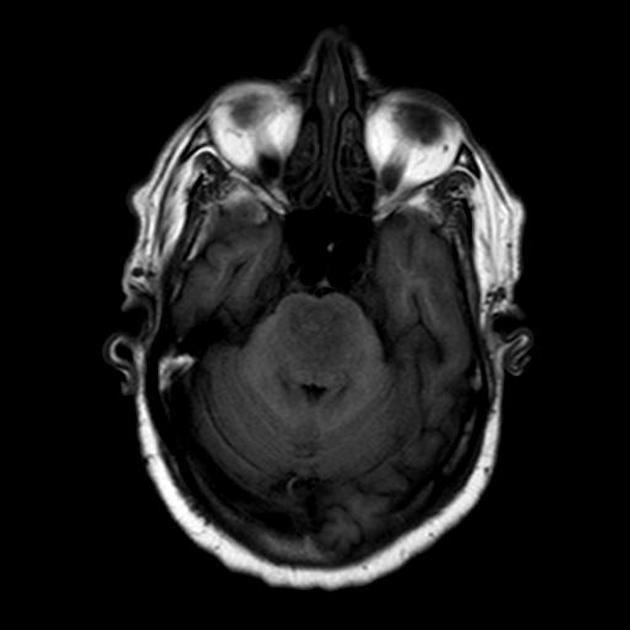
The pons is markedly expanded by a region of high T2 signal which surrounds a central area of peripheral enhancement. The center of this region is intermediate in signal on all sequences but does not restrict. No evidence of blood products.

MICROSCOPIC DESCRIPTION:
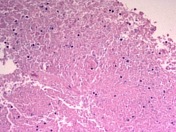
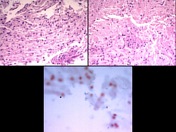
Sections of each of the three specimens submitted show small fragments of brain parenchyma. These are composed of aggregates of pontine reticular neurons with intervening glial parenchyma. There are small foci in which the glial tissue is disrupted and these areas contain prominent axonal swellings which are highlighted by neurofilament protein (NFP) immunostaining.
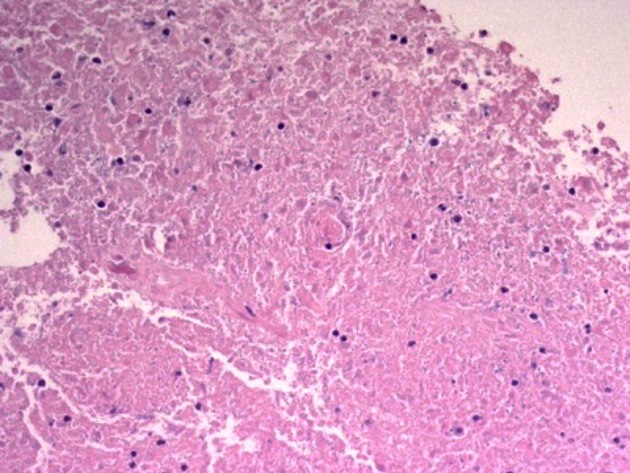
There is mild patchy reactive astrocytic gliosis. In specimen 3 there are small foci of infarct-like necrosis. These contain collection of macrophages and small numbers of neutrophils. Small numbers of Gram +ve cocci are identified in specimen 3.
There are no features of tumor. No immunostaining for SV-40/BK or Toxoplasma.
PCR TB Positive.
DIAGNOSIS:
TB abscess (PCR proven)
Reactive changes with foci of infarct-like necrosis consistent with ischemia/infarction, demyelination or infection; small numbers of Gram +ve cocci identified presumed to be contaminants; no evidence of tumor seen.
Unfortunately no sample was sent for microbiology.
The patient went on to have bronchoalveolar lavage of an area of consolidation which also revealed TB.
MICROSCOPY: Mycobacterium species.
- ANTIGEN TESTING (ON ISOLATE) MPT64 Antigen Identification Test: M.tuberculosis Complex DETECTED
- MYCOBACTERIUM CULTURE SCREEN MGIT bottle 33 days POSITIVE. Acid Fast Bacilli resemb. M.tuberculosis Complex ISOLATED
HERPES VIRUS MULTIPLEX PCR:
- CMV DNA detected
- HSV-1, HSV-2, CMV & VZV Not detected
Case Discussion
This is a interesting case, and histology of the brain biopsy in the setting of subsequent proven TB infection is most in keeping with a tuberculous abscess.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.