
Presentation
Epigastric pain.
Patient Data





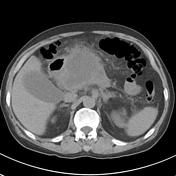
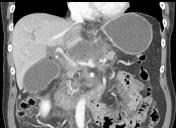
Bulky pancreas with marked retroperitoneal fat stranding, in keeping with acute pancreatitis. Lack of enhancement within pancreatic neck and proximal body are consistent with necrosis. No ductal dilatation or associated arterial or venous thrombosis. Duodenal diverticulum noted at the second part, adjacent to the pancreatic head.
Small amount of free fluid is seen in the pelvis. Small bilateral pleural effusions with bibasal atelectasis.
Conclusion: Acute pancreatitis with necrosis within the pancreatic neck and proximal body.


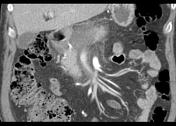
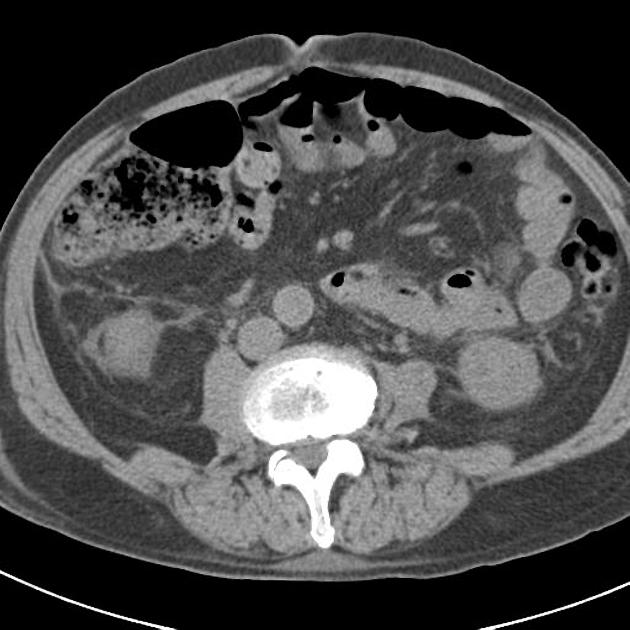
Interval development of a multiloculated fluid density cystic lesion involving the uncinate process, head and neck of the pancreas, with a thin rim of enhancement. A portion of the pancreatic head as well as the pancreatic body and tail enhance normally.
No pseudo-aneurysm identified. There is marked narrowing of the upper aspect of the superior mesenteric vein and commencement of the portal vein. In addition, the splenic vein is not clearly contrast opacified at its portal end and is likely severely extrinsically narrowed. No collaterals visible at this stage.
Mild retroperitoneal fat stranding. No lymphadenopathy. Small duodenal diverticulum. Mild intra-hepatic biliary duct dilatation involving both right and left hepatic lobes with associated dilated gall bladder. The common bile duct is non-dilated distally, measuring 5.5 mm diameter.
Conclusion: Interval development of large lesser sac / pancreatic walled-off necrosis, exerting positive mass effect upon the portal vein commencement and resulting in mild intrahepatic duct dilatation.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.