
Presentation
Headache.
Patient Data


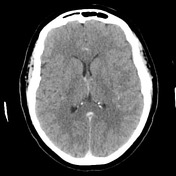
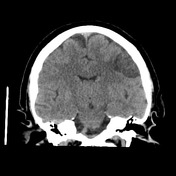
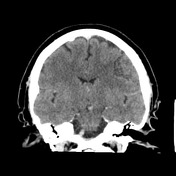
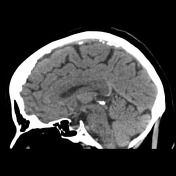

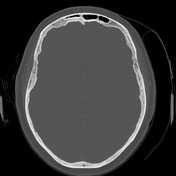


There is an extra-axial mass with broad based dural attachment at the left frontal bone, indenting the lateral aspects of the frontal lobe. It is hypodense with heterogeneous intermediate enhancement. No bony change.
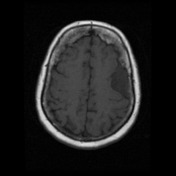

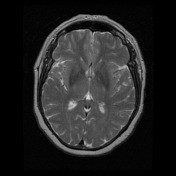
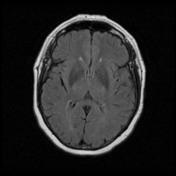
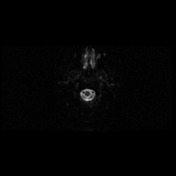
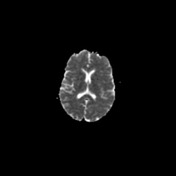
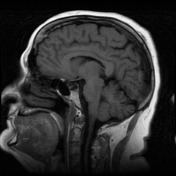
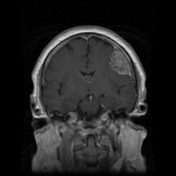
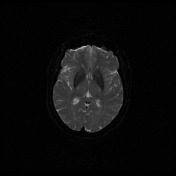
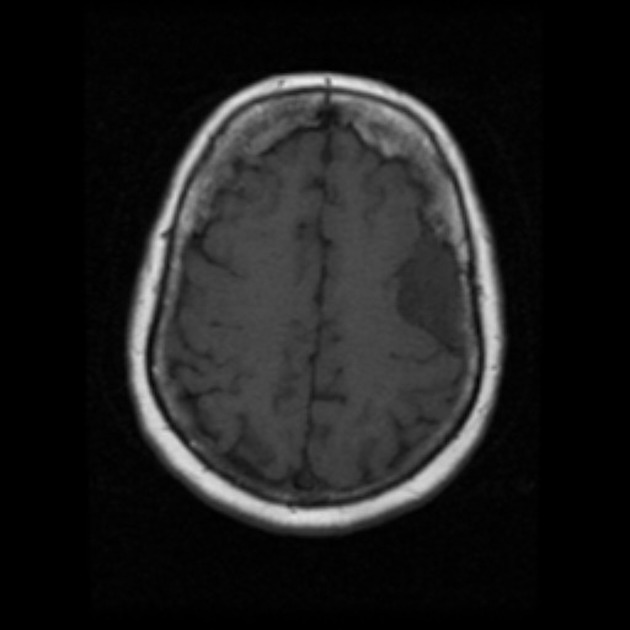
There is an extra-axial mass with broad based dural attachment at the left frontal bone, indenting the lateral aspects of the middle frontal gyrus and probably contacting the precentral gyrus inferiorly. This demonstrates heterogeneous signal intensity: predominantly hyperintense on FLAIR and T2 and hypointense on T1. It demonstrates heterogeneous enhancement following contrast administration. Diffusion weighted imaging demonstrates facilitated diffusion within the mass.
I note that there is no hyperostosis or lytic abnormality of the adjacent left frontal bone on recent CT scan.
There is a small focus of intra-axial FLAIR and T2 hyperintensity in the brain parenchyma deep to this mass.
A few small foci of FLAIR hyperintensity in the subcortical white matter of both through hemispheres probably related to chronic small vessel disease. Brain parenchyma is otherwise unremarkable. No other enhancing intra or extra-axial lesion is demonstrated. The ventricles and cortical sulci are within normal limits for a patient of this age. The major intracranial flow voids are maintained.
Conclusion:
Extra axial mass indenting left frontal lobe with minimal signal abnormality in the underlying brain parenchyma.
This most probably represents a meningioma, however the enhancement pattern, facilitated diffusion and high T2 signal are not usual. Microcystic or other histological variants of meningiomas are therefore likely. Other diagnoses (e.g. leptomeningeal metastasis) is the the other differential concern.
Case Discussion
The patient went on to have a craniotomy and resection.
Histology
MICROSCOPIC DESCRIPTION:
The sections show a moderately hypercellular meningioma. This is intensely vascular and shows a mixture of meningothelial and microcystic architectures. Tumor cells show moderate nuclear and cellular pleomorphism. An occasional mitotic figure is identified (1/20HPF). No areas of necrosis are identified and there is no evidence of brain invasion. Dural attachment is noted.
FINAL DIAGNOSIS: microcystic meningioma


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.