
Extravasation of cement into paravertebral veins in percutaneous vertebroplasty
Presentation
Non-specific abdominal pain.
Patient Data
Abdominal x-ray

Other than cholecystectomy clips, dense material is seen within the bodies of T11, T12 and L1 vertebrae. Vertical dense lines are also seen adjacent to these vertebral bodies. The bowel gas pattern is normal.
Upper abdo - CT colonogram
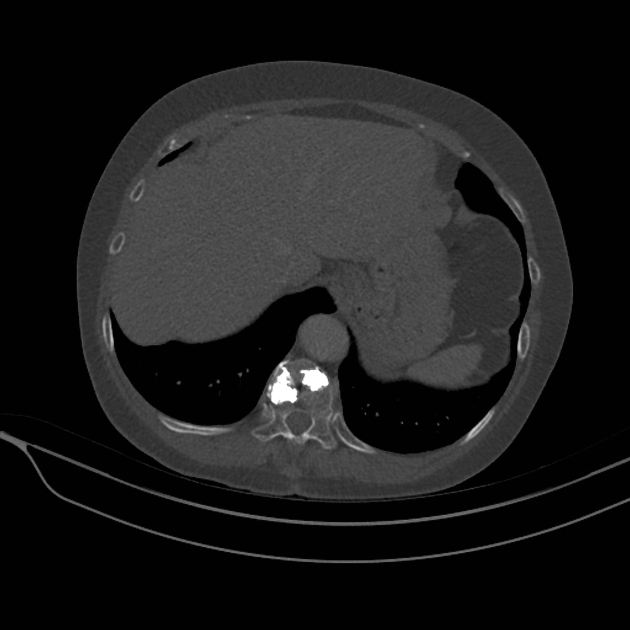
The CT confirms the presence of cement in the bodies of the T11, T12 and L1, and cement tracking into vessels adjacent to T11 and L1. No cement is seen in other vessels in the scan range, including the lungs.
Thick MIP coronal CT
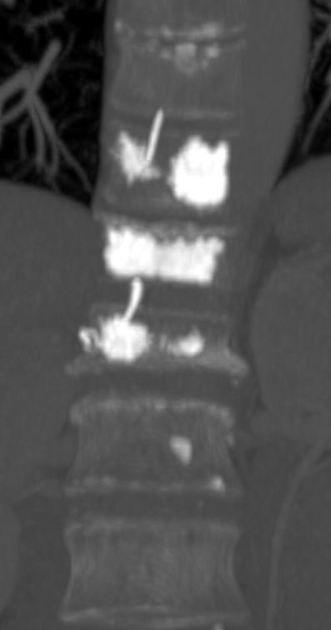
This thick MIP zoomed in image of the thoraco-lumbar junction shows the cement extravasating into paravertebral vessels at T11 and L1 levels.
Case Discussion
Cement leak at percutaneous vertebroplasty can occur into the foraminal or epidural spaces, with neurological compromise dependent on the volume of leak. Extravasation into the paravertebral veins is a potentially serious complication as it is a direct route to the right side of the heart and therefore for pulmonary embolism. Cement pulmonary emboli may be detected on post-procedure chest x-rays or CT, and may be asymptomatic if small. Reports of cerebral embolism and cardiac perforation have been published. In this case, there was no cement detected elsewhere in the body.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.