
Presentation
Low back pain. No fever. No history of respiratory disease.
Patient Data




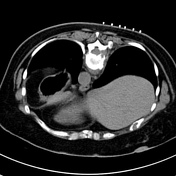
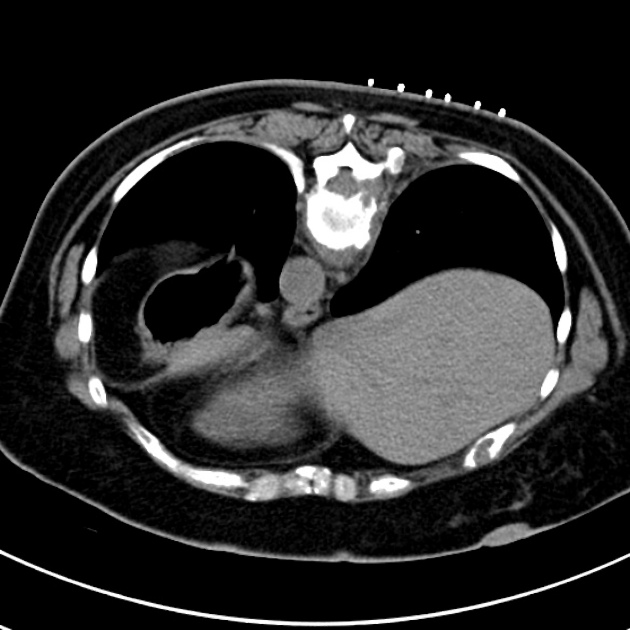
The vertebral body and right-sided posterior elements of T10 are destroyed with a large low-attenuation paravertebral component measuring up to 2 cm in depth. This extends into the central canal.
Further, there is minimal destruction of the anterior aspect of T11. The disease seems discocentric.
15mm nodule in the upper outer quadrant of the right breast.
Lungs clear.

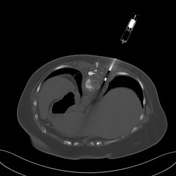
1. Surface markers applied to skin to identify best route for biopsy of the destructive T10 mass with paravertebral soft tissue elements.
2. Biopsy needle sited prior to acquisition of sample.
3. Biopsy needle in mass where sample acquired (Trucut 'pusher type' needle).
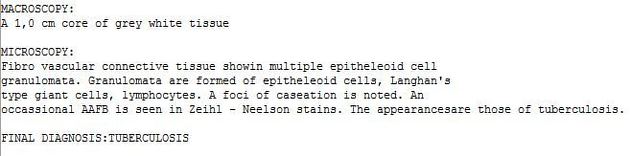
Histology from CT guided biopsy confirmed tuberculosis.
Case Discussion
TB spondylodiscitis is one of the most common manifestations of TB outside of the respiratory system. It may be relatively innocuous in presentation and radiologically appear similar to skeletal metastases. As in this case, the discocentric nature of the destruction is more suggestive of spondylodiscitis than metastases. CT-guided biopsy is one method of definitive diagnosis before treatment commencement.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.