
Presentation
2 month history of intermittent claudication.
Patient Data



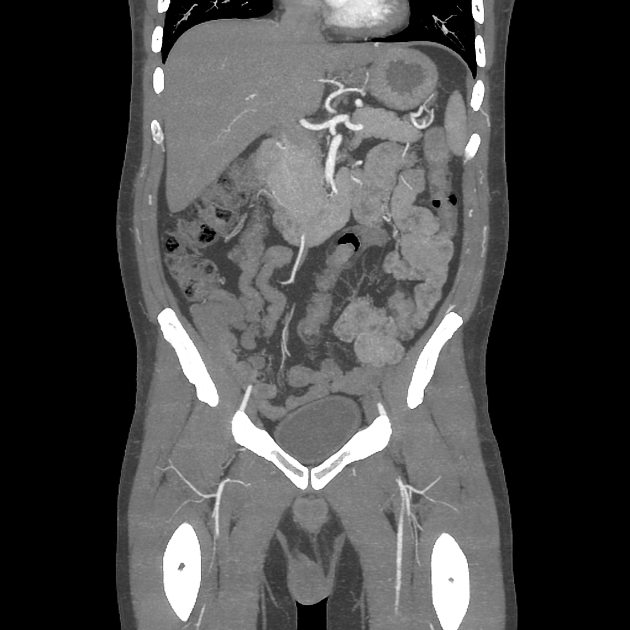
The infrarenal abdominal aorta is occluded as are the common iliac arteries and the left external iliac artery. Prominent collateral circulation can be seen supplying the inferior mesenteric, right external and internal iliac, left internal iliac and left common femoral arteries.
Case Discussion
This patient had a background of a recent acute myocardial infarct and was referred for an arterial doppler ultrasound for intermittent claudication. No arterial flow within the distal aorta was detected, which prompted this CT aortogram study.
Examination of his lower extremities reveals absent femoral, popliteal and pedal pulses bilaterally. He is now awaiting aortobifemoral bypass surgery.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.