
Presentation
Persistent pelvic pain for a few days, fever, vaginal discharge and leukocytosis.
Patient Data
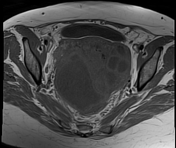

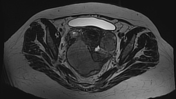
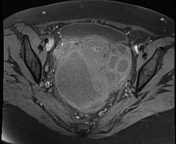
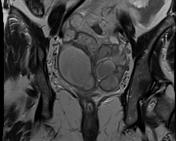
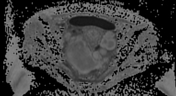
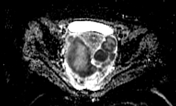

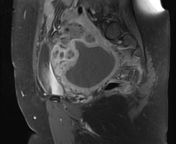
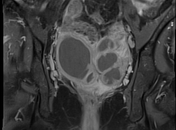
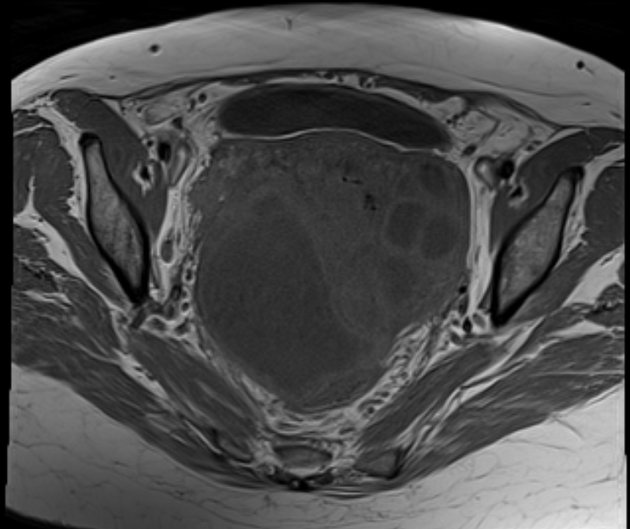
Bilateral pyosalpinx, larger on the right side, measuring 3 cm and 1.3 cm in tubal caliber for the right and left sides respectively. Both demonstrate wall enhancement and diffusion restriction. This is associated with surrounding stranding of the pelvic fat and minimal pelvic fluid.
Case Discussion
This case demonstrates tubo-ovarian abscesses with pyosalpinges and pelvic peritonitis. The ovaries couldn't be distinguished separately from the fallopian tubes.
Tubo-ovarian abscess is a late complication of pelvic inflammatory disease (PID). It is important to differentiate it from other causes of pelvic abscess like appendiceal abscess and diverticular abscess.
It can be difficult on ultrasound to differentiate the nature of the inflammatory mass and also if associated with gas formation is hard to differentiate from bowel gas.
MRI is the best choice if clinically suspecting a pelvic inflammatory mass.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.