
Presentation
Secondary school student with acute onset tetraparesis. Rapid ascending paralysis with neuromuscular weakness. Reflexes pathologically brisk. Clinically cervical myelitis. MRI on admission was normal 11 days ago.
Patient Data
Age: 12 years
Gender: Male
From the case:
Cervical transverse myelitis


Download
Info
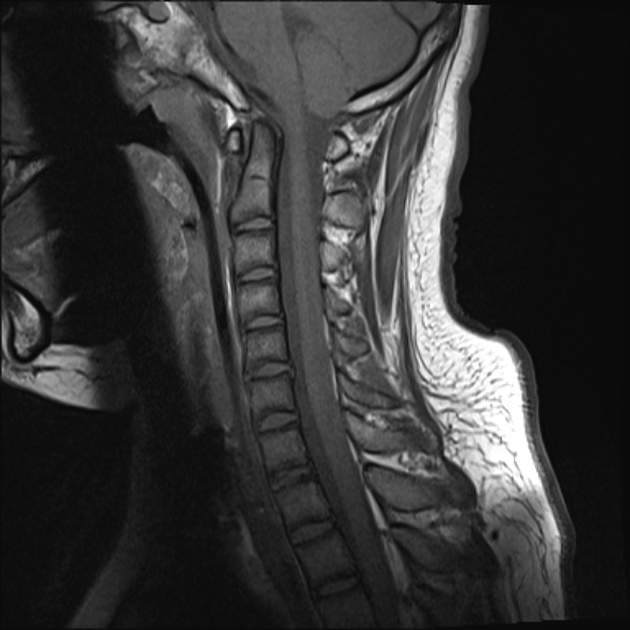
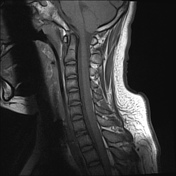
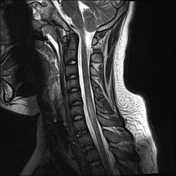
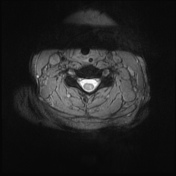
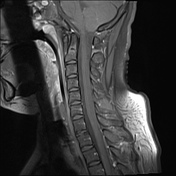
The cervical cord is expanded over a long segment between C5-T1 level with symmetrical high signal change involving both sides of the cord. Associated faint ill defined enhancement of this segment of cord.
No intradural collection.
Vertebra and disc spaces normal.
Case Discussion
A young male with MRI findings in keeping with the clinical history and examination fitting with transverse myelitis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.