
Presentation
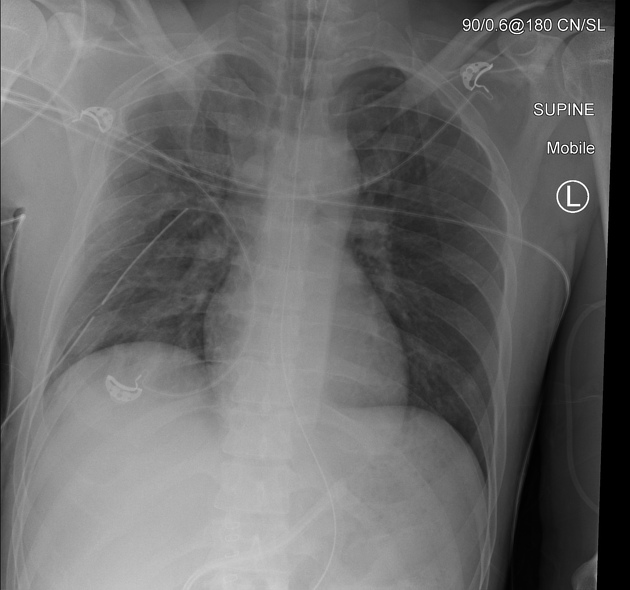
Chest x-ray post emergency trauma laparotomy.
Patient Data



Multiple displaced right sided rib fractures. Patchy increased density in the right hemithorax is probably due to pulmonary contusion. Despite presence of a right sided intercostal catheter, there is evidence of a sizable residual right pneumothorax with a deep sulcus sign. Packing is seen in the left and right upper quadrants of the abdomen related to the trauma laparotomy. ETT and NGT in situ.
Resolution of the deep sulcus on subsequent chest x-ray. Presumably the ICC was adjusted or placed on suction to assist drainage.
Case Discussion
An example of the deep sulcus sign of pneumothorax in a supine patient. This is an important chest x-ray sign, as a large volume of pneumothorax may be present in supine patients without a pleural edge being visible.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.