
Presentation
Explosion leading to an extensive laceration to the back with traumatic thoracic aorta injury treated with TEVAR. Clinically signs of anterior cord syndrome. Two days ago sudden T4 spinal at the level of T4.
Patient Data









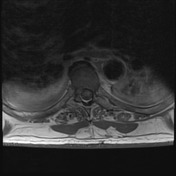
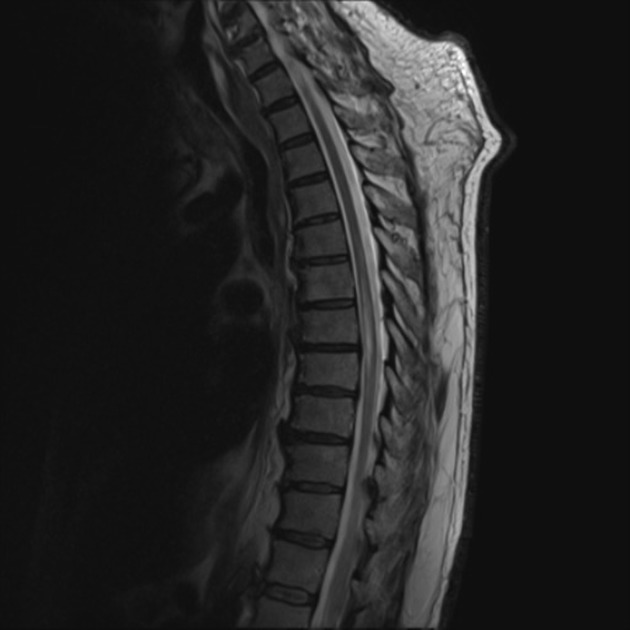
The cord demonstrates a long segment of increased T2 signal involving its anterior aspect from the level of T6 to T9, which also demonstrates diffusion restriction, consistent with anterior cord infarct. The remainder of the cord has normal caliber and signal intensity. The spinal canal and intervertebral foramina are capacious, with no high-grade stenosis identified. The thoracic spine vertebral bodies have normal height, alignment, and marrow signal intensity. Bilateral small pleural effusions noted, larger on the right. Subcutaneous edematous changes noted in the cervicothoracic dorsal region until the level of T5.



Annotated images showing the cord infarct with restricted diffusion.
Case Discussion
Imaging features are consistent with cord infarct involving the levels from T6 to T9.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.