
Presentation
Previous right mastoidectomy for acoustic schwannoma.
Patient Data


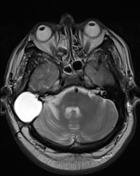
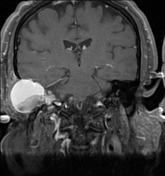


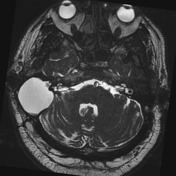

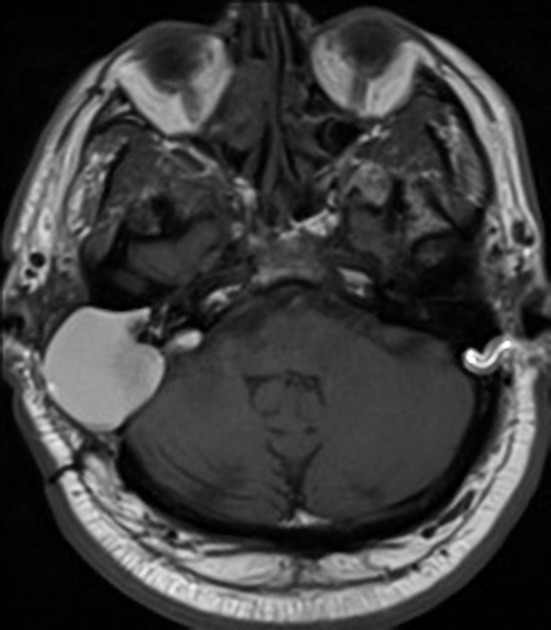
Signs of a previous right translabyrinthine surgical approach are noted. There is a cystic mass occupying the resection cavity presumed to be filled by the fat packing. It shows a high T1 signal that does not suppress on the fat-saturated sequences and also a bright T2 signal. Inspissated amorphous material forms level at the bottom of the cystic lesion. There was facilitated diffusion on DWI (not shown).
Right nasal polyp and obliteration of the right maxillary sinus were partially imaged.
Case Discussion
MICROSCOPIC DESCRIPTION: 1. Granulation tissue and fibrous tissue containing numerous elliptical cleft like spaces surrounded by a moderate inflammatory infiltrate including lymphocytes, plasma cells, eosinophils and small numbers of neutrophils. Granular brown pigment consistent with hemosiderin is present in the background. No epithelial surfaces identified. There is no evidence of malignancy. No fungi or bacteria are identified. 2. Fibrous tissue and granulation tissue with the same features as seen in specimen 1. This specimen is partially lined by an epithelial surface ranging from cuboidal to ciliated columnar. No fungi or bacteria are identified.
DIAGNOSIS: 1. Unlabelled as to site: Cholesterol granuloma. 2. Capsule lining: Cholesterol granuloma.
Right turbinectomy was also performed confirming inflammatory polyp.
This case illustrates the formation of a cholesterol granulomas years after translabyrinthine surgery.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.