
Presentation
Leg weakness.
Patient Data


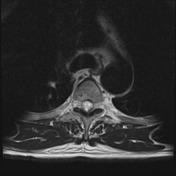

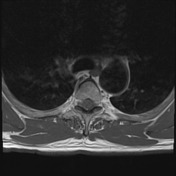


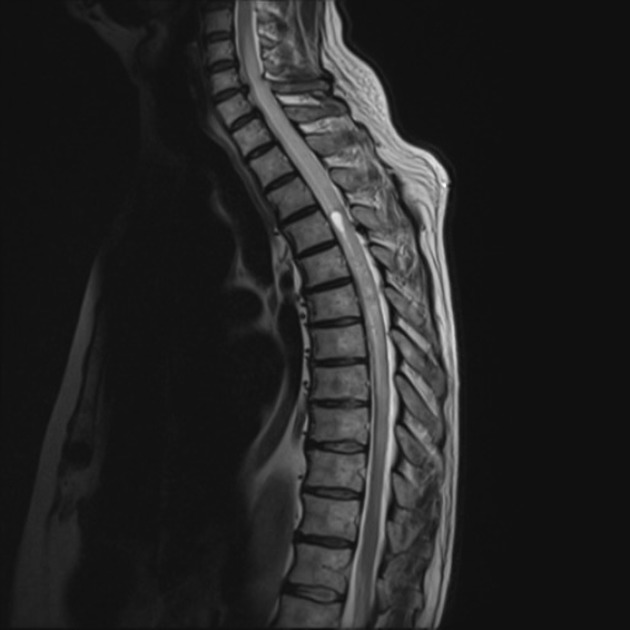
A vividly enhancing intramedullary mass is located at T6 occupying almost the entire spinal canal. It is associated with extensive high T2 signal within the cord extending to the mid-cervical cord and down to the level of T9. At the level of T4 a small focal syrinx is present.
In addition to the vividly enhancing component, both above and below it is intramedullary curvilinear enhancement with matching T2 signal loss suggestive of vessels. Superficial enhancement probably representing engorged leptomeningeal veins rather than leptomeningeal deposits although the latter is certainly a possibility.
Conclusion: The lesion almost certainly represents a tumor, and in the absence of known metastatic disease, presumably a primary tumor of the spinal cord. Prominent vessels suggests that this is a hemangioblastoma, although other entities could have a similar appearance (e.g. ependymoma - although lacking peritumoral cysts or hemosiderin capping; diffuse astrocytoma - usually enhancement is less intense and circumscribed; primary CNS lymphoma - although usually is of lower T2 signal).

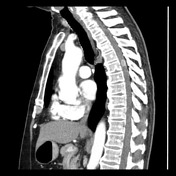

CT of the chest and abdomen (not shown) performed to examine for the possibility of metastatic disease demonstrates a vividly enhancing lesion in the thoracic cord. No primary malignancy or evidence of metastases.
Case Discussion
The patient went on to have a biopsy. At surgery, the dura was opened and the cord resembled a vascular malformation with many very prominent vessels.
Histology
Sections show a well-circumscribed tumor composed of abundant small thin-walled capillary sized blood vessels. The intervening stroma contains stellate cells with "bubbly" vacuolated cytoplasm. There is no necrosis, mitoses or atypia seen.
Immunohistochemical results show stromal cells stain: Inhibin+, 8100+ and CAM5.2-; consistent with hemangioblastoma.
FINAL DIAGNOSIS: hemangioblastoma (WHO Grade I).
Discussion
The spinal cord, due to its morphology, constrains pathology to a ~10-20 mm cylinder. As such the morphology of lesions is less helpful than in the brain. In this case, the prominent vessels are very helpful in suggesting the diagnosis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.