
Presentation
Initial episode of left eye pain attributed to corneal ulcer. Painfree after that. Developed progressive left ophthalmoplegia that became increasingly complex in pattern, and also facial nerve symptoms.
Patient Data


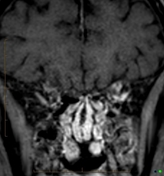
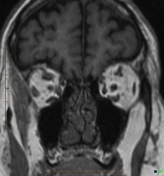
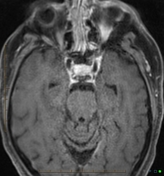
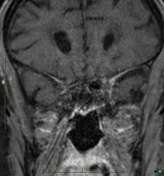
Asymmetrical increase in enhancement and bulk of the left cavernous sinus, extending laterally into superior orbital fissure, and into orbital apex.
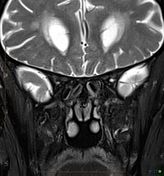
Atrophy and edema (denervation or inflammation) of all extraocular muscles on the left. Asymmetrical increase in enhancement and edema in orbital fat.
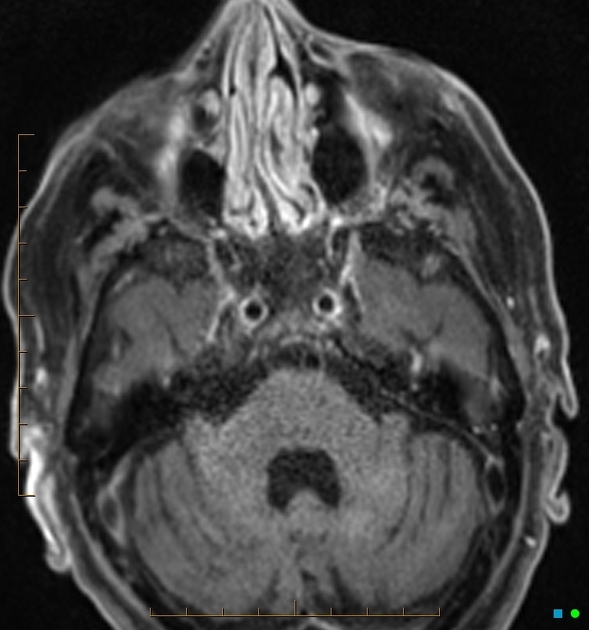
Asymmetrical increase in enhancement of the left facial nerve along its horizontal segment within petrous bone.
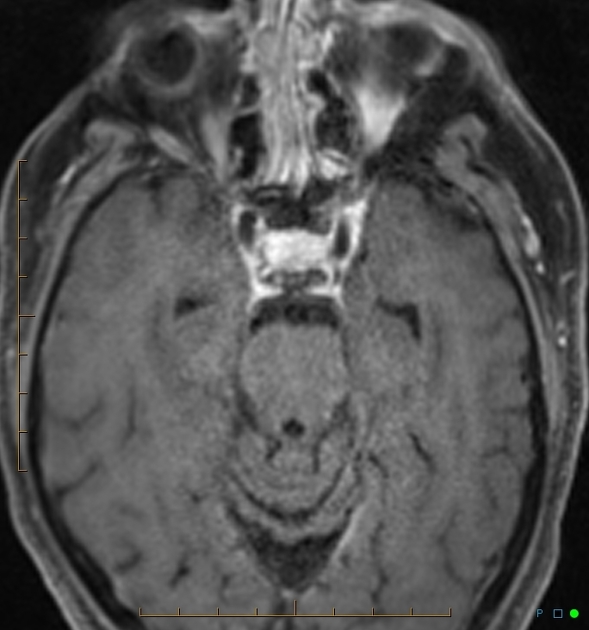
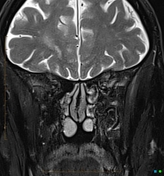
This is the study done 1 year earlier. Back then patient only had left abducens palsy.
Left cavernous sinus and superior orbital fissure enhancement were less, but present in retrospect. The edema in extraocular muscles and orbital fat were present, but subtle. No muscular atrophy back then.
Case Discussion
MRI and clinical features are suggestive of Tolosa-Hunt syndrome. Pain at the beginning, but lack of pain afterwards, is unusual, hence the delay in diagnosis. Involvement of the facial nerve is unexpected.
Sarcoid workup was negative. Lymphoma can give a similar appearance, but the clinical time course would be less typical.
The MR done on the first presentation has subtle findings. Would you have called it based upon isolated abducens palsy without other clinical cues?
Meningioma remains a differential diagnosis, even though no hyperostosis is seen.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.