
Presentation
Polyhydramnios. Previous personal, familial and obstetrical history is not relevant.
Patient Data


Our US examination from 25 weeks and 27 weeks revealed unusual echoic spots that do not look like facial bones.


US follow up at 31 weeks of pregnancy revealed mass grew up rapidly and was now protruding out of the oral cavity, pushing down and out the tongue. It was a solid mass with some internal echos, most likely calcifications or ossifications.



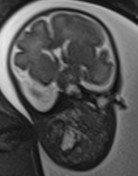

MRI showed the extension of the mass, filling both the oropharynx and nasopharynx, and also protruding through the base of the skull next to the pituitary fossa. (Probably through foramens around the sphenoid bone, such as the ovale foramen or the round foramen).


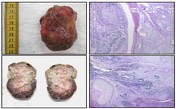

Fetopathology examination revealed a tumor arising from the nasopharynx / cavum, protruding through the oropharynx and oral cavity, and also invading the central base of the skull around the pituitary fossa. The fetus itself had normal morphology otherwise, and a mild IUGR (-2 WG).
Histology of the tumor showed a mix of epithelial, bone, chondroid and immature nervous tissues.
Case Discussion
The fetus then died in utero at 32 weeks gestation. Placental examination revealed a massive retroplacenteal hematoma, probably the cause of intrauterine death.
Fetopathology examination revealed a tumor arising from the nasopharynx (cavum), protruding through the oropharynx and oral cavity, and also invading the central base of the skull around the pituitary fossa. The fetus itself had normal morphology otherwise and a mild intrauterine growth restriction (-2 weeks gestation).
Histology of the tumor showed a mix of epithelial, bone, chondroid and immature nervous tissues.
Our final diagnosis was nasopharyngeal immature teratoma, also called epignathus teratoma.
Thanks to my dear colleagues Dr Fabrice Cuillier, Dr Marie Balu, Dr Carla Fernandez.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.