
Presentation
Urinary retention and bilateral flank pain. Labs show evidence of acute kidney injury (AKI) with leukocytosis.
Patient Data


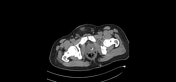


There is bilateral hydroureteronephrosis likely attributed to urethral calculus, at membranous region measuring around 7.2 mm (HU around 1200) causing distension of the urinary bladder and ballooning of the prostatic urethra.
Bilaterally perinephric and periureteric fat stranding. Superimposed infection cannot be ruled out.
Right pelviureteric junction calculus measuring around 6.5 mm (HU= 700).
Multiple bilateral renal calculi mainly at the lower poles.
Trace of free fluid noted at the pelvic region.
Case Discussion
Urethral stones are not very common. They are usually solitary and occur secondary to a lodged stone while passing from kidneys or bladder. However, they can rarely present primarily such as in a region of urethral stricture. Symptoms differ usually according to the size of the stone. If large enough; they can cause significant obstruction leading to urinary retention, hydronephrosis or renal failure.
This patient was treated by Cystourethroscopy, Laser Lithotripsy, and double J stent insertion.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.