Presentation
Head trauma. MVA.
Patient Data
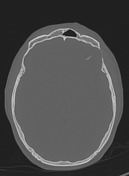

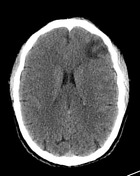


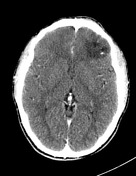
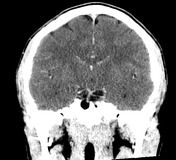
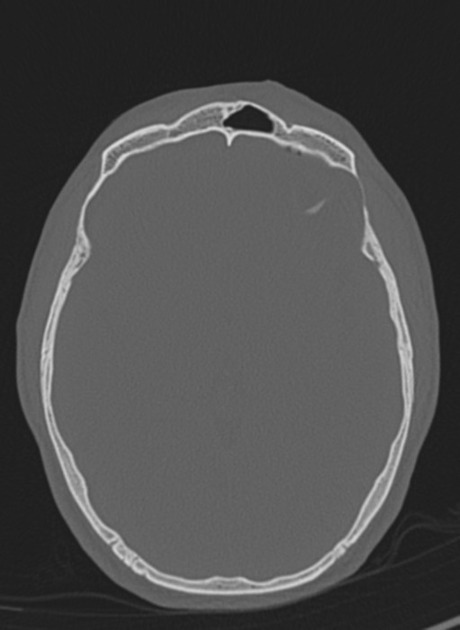
There is a comminuted fracture of the roof of the left orbit. Several curvilinear calcifications in the parenchyma of the inferolateral left frontal lobe are not bone fragments but rather intrinsic to the brain, embedded within an area of low attenuation with mass effect. The features are those of a coincidental brain tumor, presumably an oligodendroglioma.

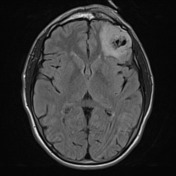
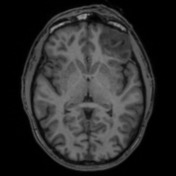
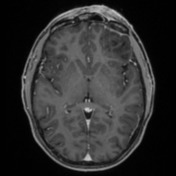
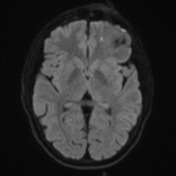
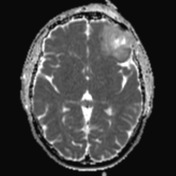
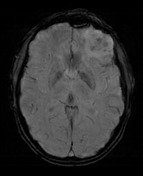
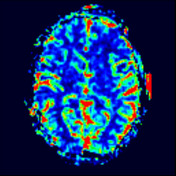
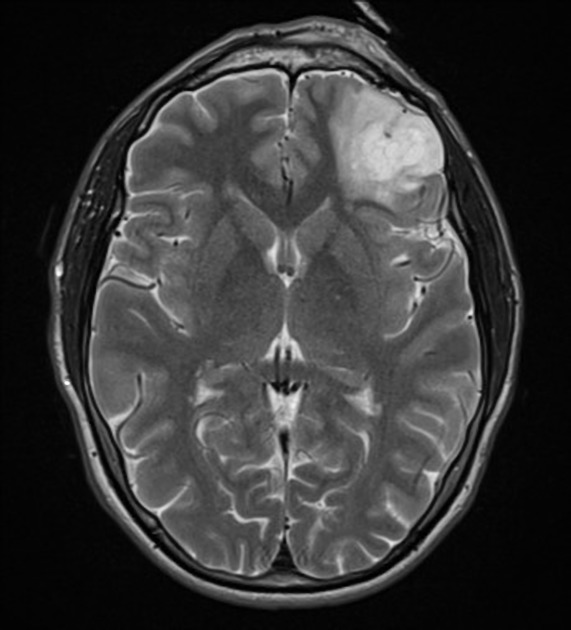
Intra-axial, cortically based lesion at the left frontal lobe demonstrates heterogeneous hypointensity on T1 and hyperintensity on T2-weighted sequences with a small central area of signal suppression on FLAIR sequences. Internal susceptibility artefact corresponds with curvilinear calcification seen on previous CT. MR spectroscopy demonstrates a reversed choline:creatinine ratio decreased NAA and increased myoinositol. Several vessels traverse the lesion, and this is also seen on perfusion sequences, although there is no contrast enhancement otherwise.
Orbital roof fractures are better seen on previous CT, associated with periorbital edema.
Conclusion:
Left frontal lobe mass is favored to represent oligodendroglioma given its size, presence of calcification and traversing vessels, and central cystic changes. Other differentials include dysembryoplastic neuroepithelial tumor or low-grade astrocytoma.
Case Discussion
The patient went on to have a resection.
Histology
Sections of cerebral cortex and white matter show a hypercellular tumor with a fibrillary background also containing small thin-walled vessels and scattered calcifications. Tumor cells have round nuclei with speckled chromatin and perinuclear clearing. Occasional mitoses are present, up to 3 per 10 high-powered fields. There are areas with microvascular proliferation and focal palisading necrosis.
IMMUNOHISTOCHEMISTRY:
- GFAP: Background staining
- IDH-1 R132H: Positive (mutated)
- ATRX: Intact (non-mutated)
- p53: Negative
- p16 CDKN2A: Patchy staining
- Ki67: Up to 10%
SEQUENCING:
- 1p/19q codeletion: DETECTED
- EGFR amplification: Not detected
- IDH1 codon 132: PATHOGENIC VARIANT DETECTED (R132H)
- IDH2 codon 172: No pathogenic variant detected
FINAL DIAGNOSIS:
oligodendroglioma, IDH-mutant, and 1p/19q-codeleted (WHO CNS5 grade 3)


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.