
Presentation
Bilateral hearing loss follow-up.
Patient Data


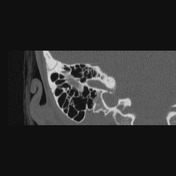
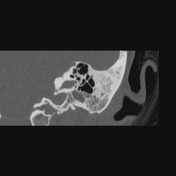
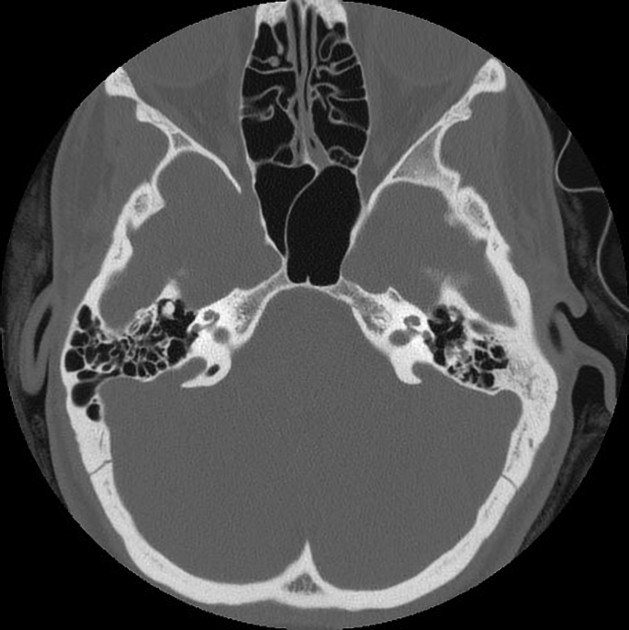
Bilateral dilation of vestibular aqueducts associated with the bilateral absence of posterior semicircular canal (aplasia). Cochleae have an anatomical appearance with more than two turns, and the bony modiolus is appreciated bilaterally. There is no significant labyrinth abnormality bilaterally.
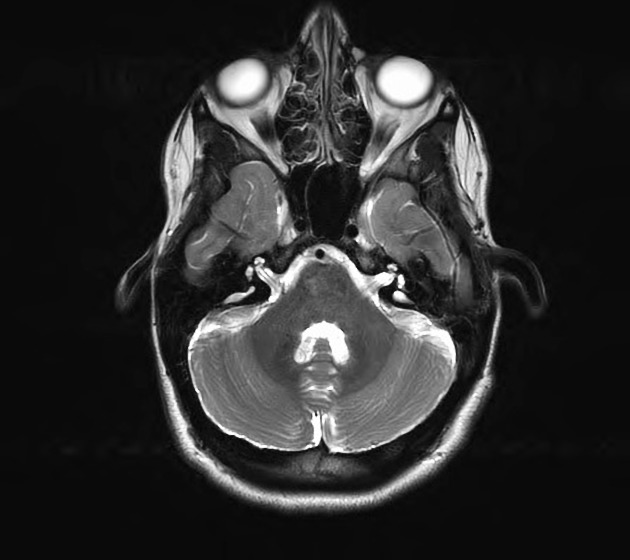
The patient was evaluated 6 years after for a new onset of atypical migraine and aura with MRI and MRA studies. No intracranial parenchymal, meningeal or vascular abnormality was identified.
Bilaterally dilated vestibular aqueducts are redemonstrated as T2 hyperintense structures in the posterior aspect of the temporal petrous pyramids and lateral to internal auditory canals. Left lower mastoid T2 hyperintensities correspond to left mastoid partial opacities in the CT, most likely serosal fluid accumulation.
Case Discussion
The vestibular aqueduct extends from the posteroinferior surface of the temporal petrous to the medial wall of the vestibule and contains the endolymphatic duct that connects the endolymphatic sac to the utricle and saccule.
Enlarged vestibular aqueduct syndrome (EVAS):
neurosensorial hearing loss in the context of vestibular duct enlargement more than the posterior semicircular canal which runs parallel and anterior to it
the most common cause of congenital sensorineural hearing loss in children and young adults with a female-to-male ratio of 3:2 and being bilateral in 50-60% of patients
coexisting with semicircular canal abnormalities but highly associated with cochlear anomalies including Mondini malformations. Vestibular aqueduct formation and the portioning of the cochlea are at the last stages of development of the inner ear in which both structures might be affected by a teratogenic insult
high-resolution temporal bones CT demonstrates the bony outline of the vestibular aqueduct; but MRI (T2WI for vestibular aqueduct) further identifies the integrity of the cochlea, the cochlear nerve, and the fluid-filled spaces of the inner ear as well as associated parenchymal or vascular abnormalities
precise assessment and description of cochlear anomalies are necessary as they might change the management including surgical intervene or cochlear implantation
Case contributed by Dr. Lorne Rosenbloom, neuroradiology assistant professor of McGill University.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.