
Presentation
Occipital swelling since birth.
Patient Data
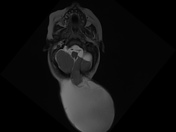

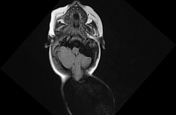

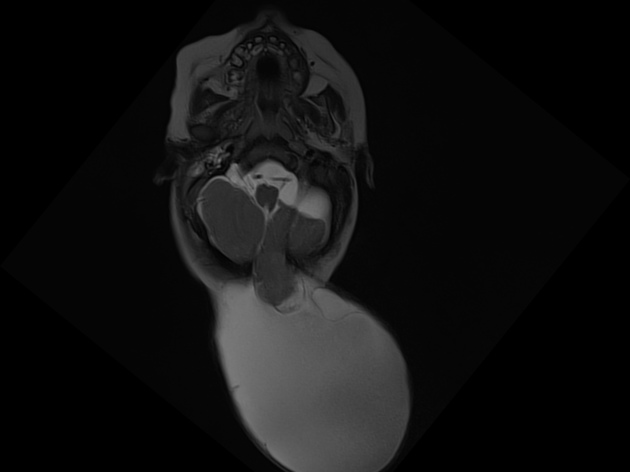
MRI brain shows midline occipital bony defect (1.9 x 1.6 cm) with herniation of cerebellar vermis and portion of left cerebellar hemisphere through the defect. The herniated brain parenchyma is surrounded by large CSF intensity fluid collection (9 x 11 x 9 cm). These features are consistent with large occipital meningoencephalocele.
There is traction on posterior fossa structures with anteroposterior elongation of fourth ventricle, resulting in moderate bilateral lateral and third ventricular dilatation.
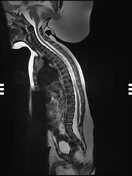

Low lying tethered cord is noted, tethered to the posterior surface of L5 spinal canal. No mass lesion is noted at the level of tethering.
Case Discussion
Occipital encephalocele and meningoencephaloceles can occur in isolation or can be part of syndromes, like Meckel-Gruber syndrome. Early antenatal detection can be done with careful transverse sweeps across the fetal skull.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.