
Presentation
Cough, sputum, fever, and hemoptysis for one year.
Patient Data
Age: 25 years
Gender: Female
From the case:
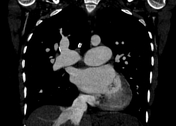
Double inlet left ventricle (DILV) with d-TGA



Download
Info
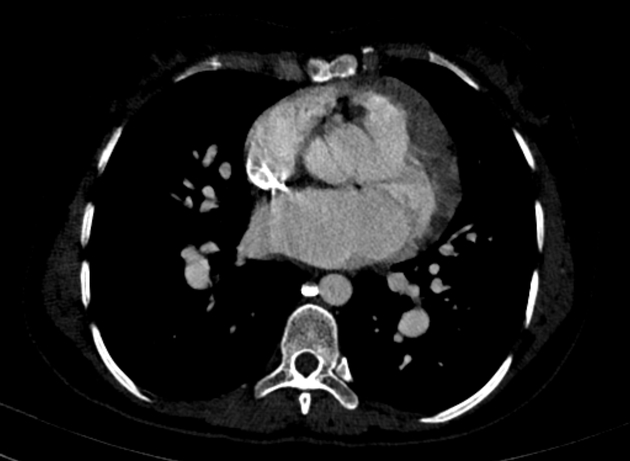
- dominant subpulmonary ventricle connected to both atrioventricular valves
- anteriorly located small subaortic outlet chamber with no atrioventricular connection
- ventriculoarterial discordance with the aorta arising from the small subaortic outflow chamber and the dilated pulmonary trunk from the dominant ventricle
- ventricular septal defect with a connection of the dominant ventricle and the hypoplastic anterior chamber
- hypoplastic aorta
- dilatation of the pulmonary trunk (49 mm) and bilateral pulmonary arteries as well as the lobar and segmental branches
- significant dilatation of the normally located right atrium and left atrium
- early reflux of contrast is seen in the IVC and hepatic veins
Case Discussion
Single ventricle physiology in keeping with a double inlet left ventricle and transposition of the great arteries (d-TGA) and associated Eisenmenger syndrome.
A case like this poses many diagnostic difficulties:
The smooth septal side of the single-chamber suggests the double inlet left ventricle, which gives rise to the dilated pulmonary artery and a connection to the small subaortic accessory chamber representing the hypoplastic right ventricle. The latter is positioned anteriorly (right) as opposed to posteriorly (left) suggesting a d-loop configuration.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.