
Presentation
Gradual speech and gait problems with decreased cognition.
Patient Data




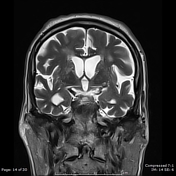

The midbrain to pons ratio (PSP) measures about 0.19 (normally >0.24), giving the appearance of a "hummingbird sign" on midsagittal images.
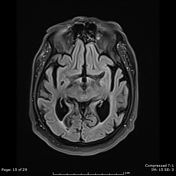
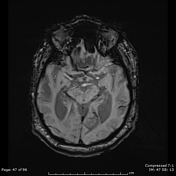
Magnetic resonance parkinsonism index measures about 14.56 (normally <13.55), with thinning of the superior colliculi, more on the left side.
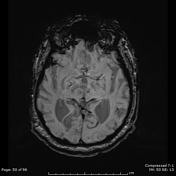
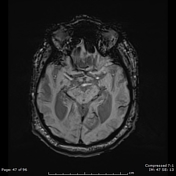
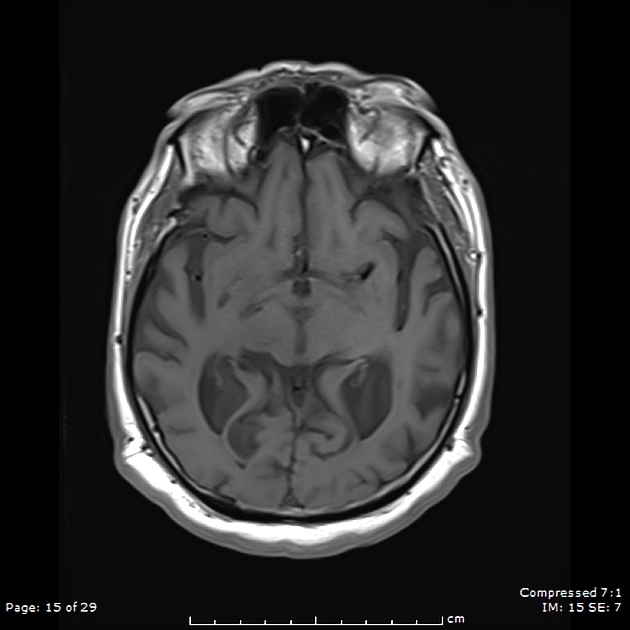
Concave dorsolateral midbrain margin and deep interpeduncular cistern, giving the "Mickey Mouse appearance".
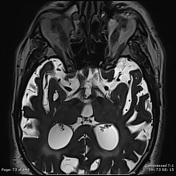
Diffuse cerebral and cerebellar atrophic changes are noted, along with dilatation of all ventricles.
Features are collectively compatible with a primary tauopathy, likely progressive supranuclear palsy.
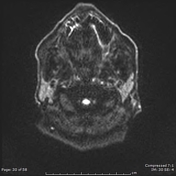
Faint tiny focus of diffusion restriction in the left temporal periventricular white matter, suggesting acute/subacute infarct.
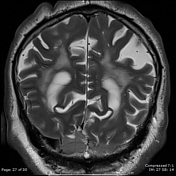
Confluent bilateral periventricular T2/FLAIR hyperintensity reaching the bilateral centrum semiovale, suggesting Fazekas 3 microvascular ischemic disease.
Case Discussion
Although certain features help in favoring progressive supranuclear palsy (PSP) over alternative clinical diagnoses (Parkinson disease and multiple system atrophy), it should be noted that except in classical cases, imaging features can usually at most be suggestive of the diagnosis rather than pathognomonic, as there is overlap with other conditions.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.