
Presentation
Hypertensive and diabetic undergoing investigations for recurrent transient ischemic attacks.
Patient Data
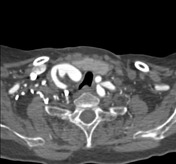


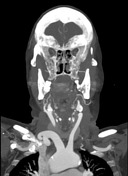
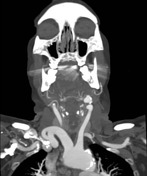

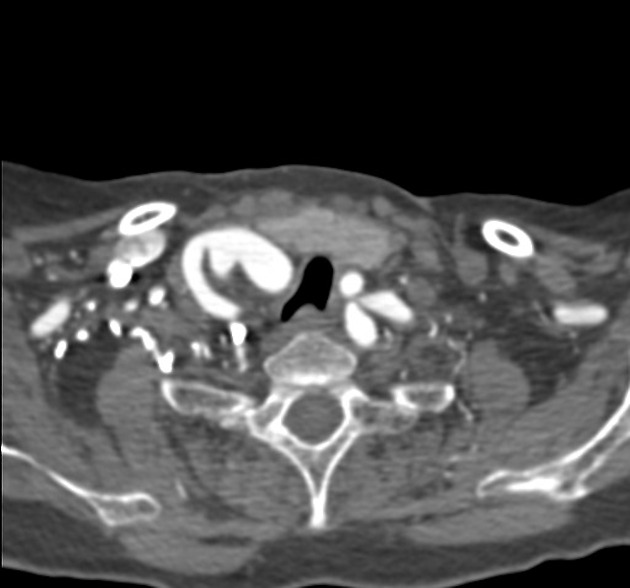
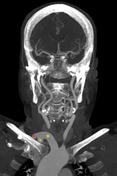
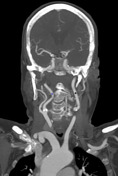
Elongated brachiocephalic trunk, measuring about 4 cm in length, bifurcating into the right common carotid and subclavian arteries above the level of the right sternoclavicular joint. It appears to compress the right thyroid lobe, indenting the upper airway with mild contralateral deviation. Findings are in keeping with a high-riding brachiocephalic artery.
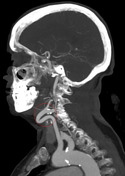
Elongation and marked anterior kinking of the left common carotid artery.
Retropharyngeal right ICA.

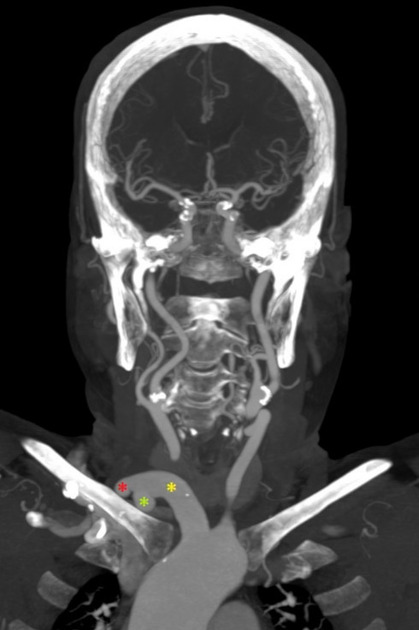
Brachiocephalic trunk (yellow asterisk)
Right common carotid (red asterisk)
Right subclavian artery (green asterisk)
Kinked left common carotid (red circle)
Retropharyngeal right ICA (blue asterisk)
Left ICA (black asterisk)
Case Discussion
The brachiocephalic artery normally bifurcates into the right common carotid and subclavian artery behind the right sternoclavicular joint. A high-riding brachiocephalic trunk bifurcates above the level of the right sternoclavicular joint and is thought to be secondary to a persistent long portion of the proximal segment of the right fourth aortic arch.
Patients can be asymptomatic or may present with a pulsatile neck mass.
In this case, patient's age, underlying hypertension and atherosclerosis, in addition to a high-riding brachiocephalic artery are possible contributing factors to the tortuous retropharyngeal course of the right internal carotid artery.
It is imperative to report such vascular abberations in order to avoid devastating intraoperative hemorrhage .


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.