
Presentation
Months of proximal calf pain.
Patient Data
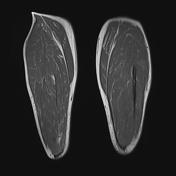

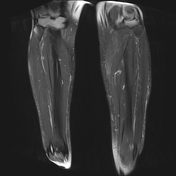
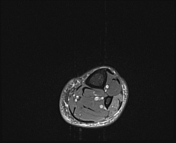
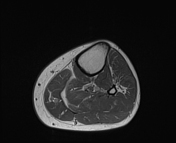
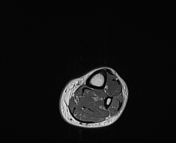
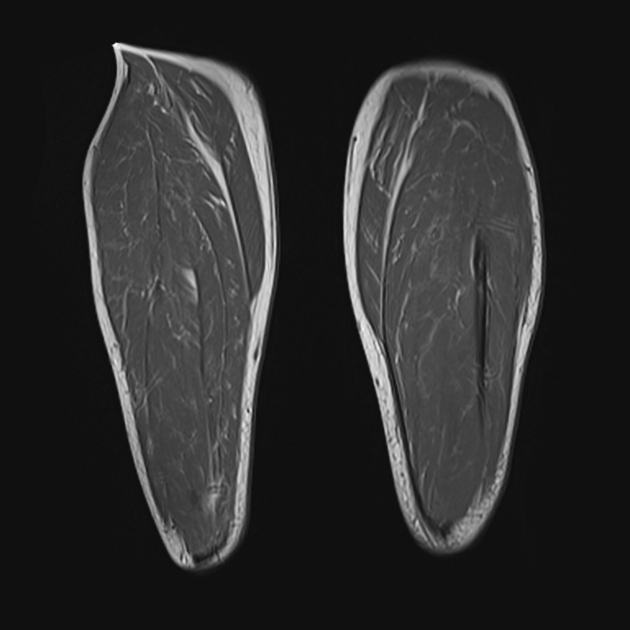
Left more than right mild subcutaneous edema with prominent deep veins, with fluid fluid levels suggestive of sluggish flow or stasis. Short saphenous vein is not dilated and there are no superficial varicosities.
Mild high signal in the inferior aspects of the gastrocnemius muscles bilaterally without feathery muscle edema.
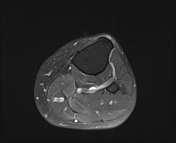
Small left knee joint effusion with severe chondromalacia patellae.
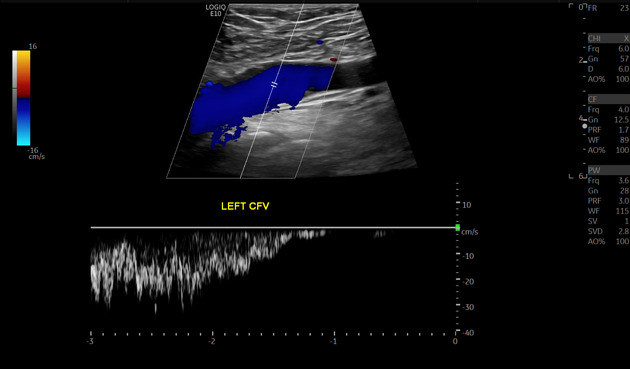
The saphenopopliteal junction was incompetent. Short saphenous vein incompetent from saphenopopliteal junction to 10cm below knee crease. Saphenofemoral junction competent. Great saphenous vein competent. No deep venous incompetence. No incompetent perforator
Case Discussion
Vascular causes of leg pain should be considered and vascular structures should be included as a check area on musculoskeletal MRI. The dilated veins with fluid-fluid levels are the key finding. The muscle edema is probably related to venous hypertension.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.