
Afferent loop syndrome - secondary to incarcerated trocar site hernia
Presentation
Laparoscopic Roux-en-Y Gastric Bypass in two weeks, presented with abdominal pain, distention & N/V.
Patient Data



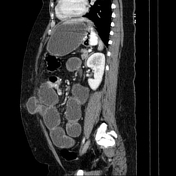

- Evidence of Roux-en-Y gastric bypass with distal jejunojejunostomy anastomosis, with the length of bypassed jejunal loops being longer than usual.
- Moderate to severe dilatation of gastric remnant and biliopancreatic (afferent) limb up to its distal part.
- An incarcerated jejunal loop (proximal to jejunojejunostomy anastomosis) through a left paramedian anterior abdominal defect (trocar site), with slight wall thickening and peripheral fat stranding of the incarcerated bowel loop.
- Collapsed loops of the biliopancreatic limb distal to the herniation site.
- Patent ante-colic Roux limb with oral contrast in small bowel loops and colon.
- Mild intra-abdominal fluid (Interloop).
Findings are consistent with biliopancreatic (afferent) limb obstruction secondary to an incarcerated incisional (trocar site) hernia.
Promptly, the patient underwent surgical release of the incarcerated bowel loop.
The length of bypassed jejunal loops was about 250cm, there was no sign of bowel wall ischemia at surgery.
Eventually, the patient was discharged without any complications.
Case Discussion
This case demonstrates a patient presenting with biliopancreatic (afferent) limb obstruction secondary to a trocar site incisonal hernia in the early postoperative period.
Any intra-abdominal surgical procedure can be followed by a small bowel obstruction. In bariatric surgeries, it can occur secondary to adhesions, technical errors during surgery, and hernias (internal and incisional), although it is an uncommon complication within the early postoperative period (30 days). Usual causes in this subset of patients include trocar site incisional hernia and internal hernias, secondary to inadequate fascial repair.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.