
Presentation
Sudden onset of chest pain and shortness of breath. Collapsed in emergency department.
Patient Data


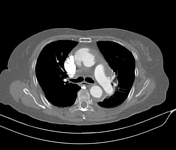


A dissection aortic intimal flap seen arising in the ascending aorta distal to sinus of Valsava/sinotubular junction and spirals along the ascending aorta, aortic arch till descending thoracic aorta distally at T11 vertebral level. It forms large false lumen at the right anterolateral aspect of ascending aorta and at left posterolateral aspect of descending aorta.
Dilatation of the ascending aorta fits the definition of aortic aneurysm with location of intimal tear at the 9 to 12 o'clock (viewing the ascending aorta at cross sectional/axial cut). The intimal tear is located proximal to the origin of right brachiocephalic trunk.
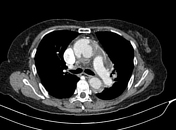
Active contrast extravasation can be witnessed into the false lumen during arterial phase and delayed pooling of contrast into the pericardial space during portovenous phase in keeping with hemopericardium. A small round shaped thrombus/filling defect within the false lumen near to the intimal tear.
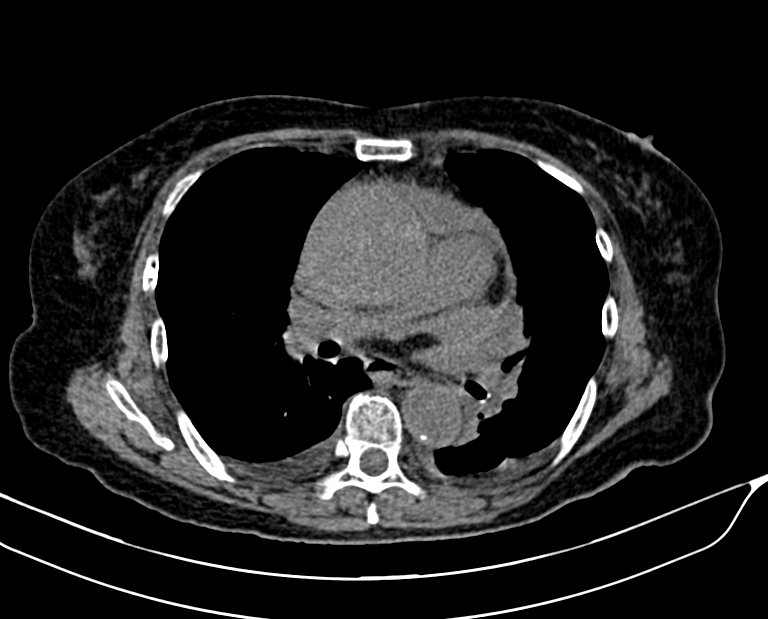
Pericardial effusion without pericardial thickening. The content of pericardial effusion is high attenuating measuring 35-40HU. Reflux of contrast material into inferior vena cava and hepatic veins during arterial phase. Reflux of contrast is also noted into the azygous vein. Inversion of the right ventricular wall noted. These CT features are in keeping with cardiac tamponade.
Some relevant measurement:
1. Aortic root: 2.6cm
2. Sinus of Valsava: 3.2cm
3. Sinotubular junction: 3.5cm
4. Mid ascending aorta: 5.1cm (abnormal aneurysm)
5. Aortic arch: 3.5cm
6. Descending thoracic aorta: 3.0cm
Severe grade of coronary arteries calcification, right coronary artery arises from anterior cusp and left side from left cusp. They are from true lumen.
No extension of the aortic dissection into the right brachiocephalic trunk, left common carotid artery and left subclavian artery.
No periaortic or mediastinal hematoma.
Bilateral minimal pleural effusion with adjacent passive lung atelectasis in both lower lobes.
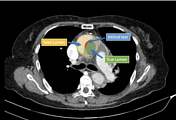
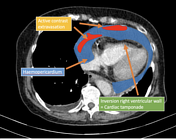
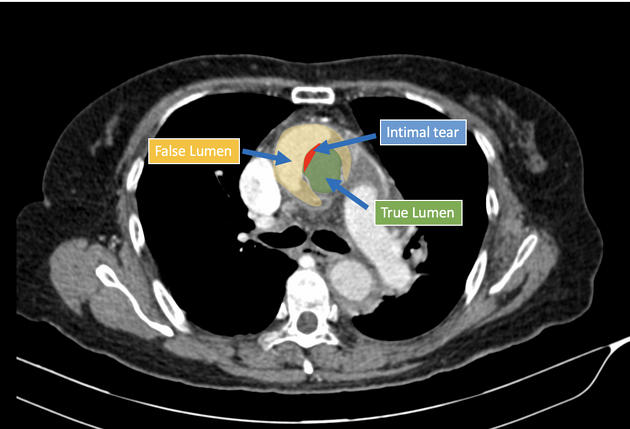
Annotated images showed the false lumen, true lumen, intimal flap and hemopericardium.
One week ago, patient has 2-day hospital admission and treated as unstable acute coronary syndrome (ACS) and discharged with double anticoagulants.
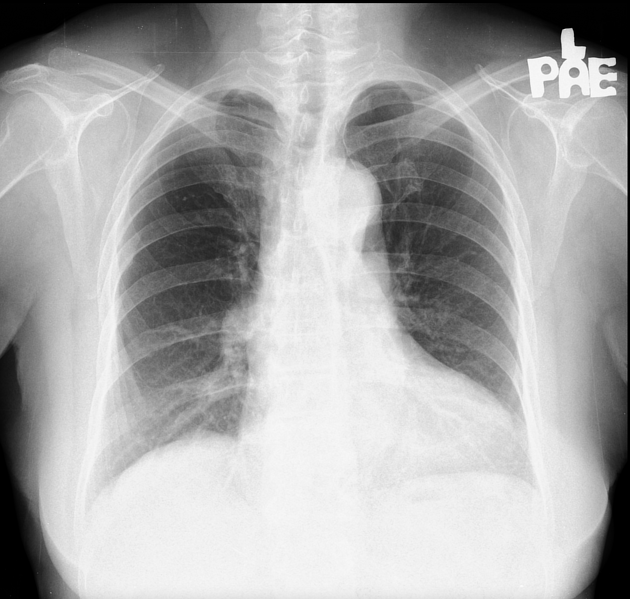
Borderline cardiomegaly with normal mediastinal width in chest radiograph performed one-week ago during last hospital admission.
Latest chest radiograph during this admission.
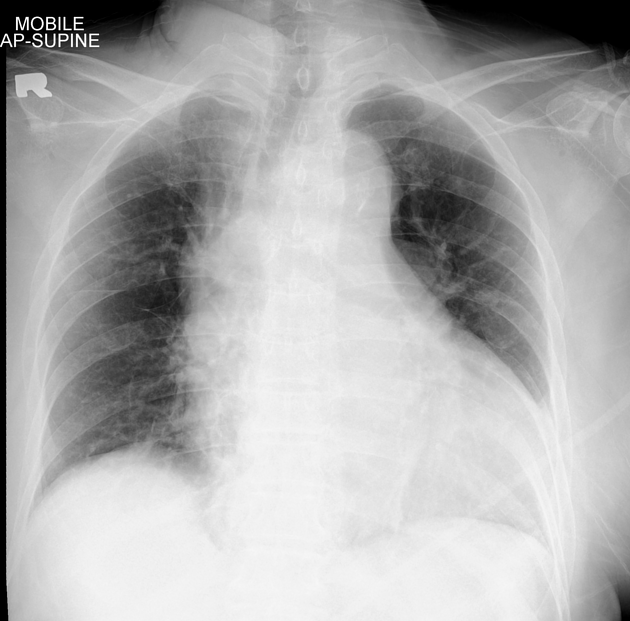
Comparing to the chest radiograph (one week ago), significant widening of mediastinum, measuring up to 12.6cm in maximum width. Enlargement of the ascending aorta contour.
It is highly suspicious of dissecting aortic aneurysm and possible mediastinal hematoma.
Case Discussion
Stanford type A aortic dissection, complicated with ascending aortic aneurysm and cardiac tamponade secondary due to rupture into pericardium.
Active contrast extravasation into the false lumen and pericardial space via intimal tear is worrisome sign for acute expansion of hematoma.
Undeniably, aortic dissection might lead to abnormal electrocardiogram ECG and causing incorrect diagnosis of ACS.
This case showed the importance to differentiate the diagnoses between acute coronary syndrome and aortic dissection, as the treatment for ACS with anticoagulants are disastrous for aortic dissection as depicted in this case.
Comparison the basic chest radiographs will give high yield on detection of rupture of aortic dissection.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.