
Presentation
Right upper quadrant adominal pain and acute renal failure.
Patient Data



Partly calcified gallstone at the neck of the gallbladder. No pericholecystic fluid or fat stranding.
Gallbladder wall is difficult to appreciate but may be mildly thickened.
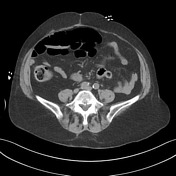
High density within a grossly dilated common bile duct is highly suspicious for choledocholithiasis.
Gas is present within the liver within portal vein branches and there is a small locule of gas within the superior mesenteric vein with more substantial volume of gas within tributaries from the mid to distal stomach.
Bowel resection noted with rectosigmoid anastomotic sutures. 3 cm right basal pulmonary mass. In the pelvis, there are loops of small bowel with fecal material mimicking mural gas - note no mural thickening, adjacent fat stranding or free fluid.
Case Discussion
Acute cholangitis is essentially a clinical diagnosis. Imaging is useful to assess for biliary tree dilatation, possible causes as well as complications. The patient proceeded to ERCP which confirmed choledocholithiasis and ascending cholangitis; it also allowed for biliary decompression.
Portal venous gas can be associated with severe abdominal sepsis such as cholangitis.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.