
Presentation
50 year old female presented with WFNS grade 3 Fisher grade 4 subarachnoid hemorrhage secondary to a left posterior communicating artery aneurysm. Aneurysm coiled acutely. Day 8 post SAH deteriorating conscious level and right hemiplegia.
Patient Data


The pre-treatment image shows vasospasm involving the left M1 and A1 segments.
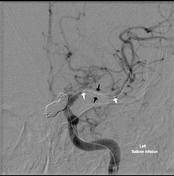
An endovascular balloon catheter has been passed through a guiding catheter in the left ICA and directed into the left M1 segment over a micro guide wire. The two markers indicate the proximal and distal extent of the balloon (white arrows). The balloon has been inflated in the middle cerebral artery (black arrows).
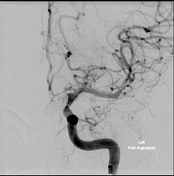
After angioplasty the left MCA is of normal caliber. Left hemisphere perfusion is significantly improved.
Case Discussion
Transluminal balloon angioplasty is an option for treatment of post subarachnoid hemorrhage cerebral vasospasm. It is an invasive procedure that carries a risk of vessel perforation (by microguidewire) or rupture (by balloon inflation). However, when successful its effects persist, in contrast to the often transient effects of intra-arterial vasospasm treatment with calcium channel blockers such as Nimodipine or Verapamil ("chemical angioplasty"). For this reason it may be employed when there is difficulty in assessing the patient clinically, e.g. in high WFNS grade subarachnoid hemorrhage when the patient might be ventilated and sedated.


 Unable to process the form. Check for errors and try again.
Unable to process the form. Check for errors and try again.